Medical Disclaimer: This is educational content only, not medical advice. Consult a licensed healthcare provider for diagnosis/treatment. Information based on sources like WHO/CDC guidelines (last reviewed: 2026-02-13).
This article is being expanded for more depth. Check back soon!
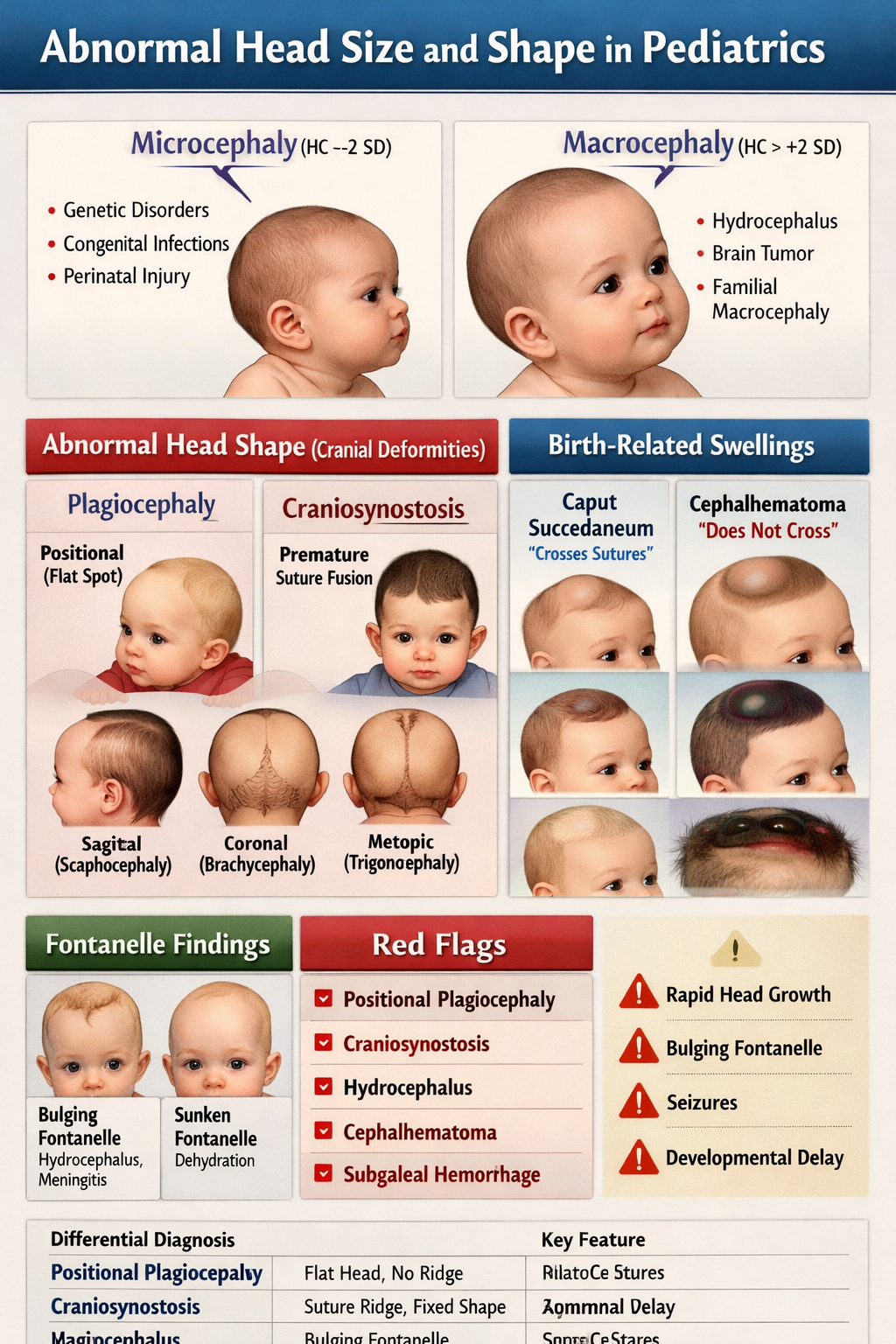
Abnormal Head Size and Shape in Pediatrics Microcephaly Macrocephaly Craniosynostosis Guide
Frequently Asked Questions
What is considered an abnormal head circumference in pediatrics?
Head circumference is abnormal when it falls below –2 standard deviations (microcephaly) or above +2 standard deviations (macrocephaly) for age and sex on standardized growth charts.
What is microcephaly in children?
Microcephaly is defined as a head circumference less than –2 SD below the mean, indicating reduced brain growth and often associated with developmental delay or neurologic impairment.
What are the common causes of microcephaly?
Common causes include congenital infections (CMV, Zika), chromosomal abnormalities, genetic syndromes, perinatal hypoxic injury, severe malnutrition, and metabolic disorders.
What is macrocephaly in pediatrics?
Macrocephaly is defined as head circumference greater than +2 SD above the mean. It may be benign familial or due to serious intracranial pathology such as hydrocephalus.
What are the major causes of macrocephaly?
Causes include benign familial macrocephaly, benign enlargement of subarachnoid spaces (BESS), hydrocephalus, intracranial tumors, subdural hematoma, and storage disorders like Tay-Sachs.
How can benign macrocephaly be differentiated from hydrocephalus?
Benign macrocephaly usually has normal development and stable growth, while hydrocephalus presents with rapid head enlargement, bulging fontanelle, vomiting, sunset eye sign, and raised intracranial pressure.
What is plagiocephaly in infants?
Plagiocephaly refers to asymmetrical flattening of the skull, most commonly positional due to prolonged supine positioning, and is usually benign.
How is positional plagiocephaly different from craniosynostosis?
Positional plagiocephaly has no suture ridging and improves with repositioning, whereas craniosynostosis involves premature suture fusion, palpable ridging, fixed deformity, and may cause raised intracranial pressure.
What is craniosynostosis?
Craniosynostosis is the premature fusion of one or more cranial sutures, leading to abnormal head shape and potential restriction of brain growth.
What are the main types of craniosynostosis and head shapes?
Sagittal fusion causes scaphocephaly, coronal fusion causes brachycephaly or anterior plagiocephaly, metopic fusion causes trigonocephaly, and lambdoid fusion causes posterior plagiocephaly.
What imaging is best for diagnosing craniosynostosis?
CT scan with 3D reconstruction is the gold standard investigation for confirming craniosynostosis and identifying the fused suture.
What is caput succedaneum?
Caput succedaneum is scalp edema present at birth that crosses suture lines and resolves spontaneously within 1–2 days.
What is cephalhematoma and how is it recognized?
Cephalhematoma is a subperiosteal hemorrhage that does not cross suture lines, appears hours after birth, and may lead to neonatal jaundice.
What is subgaleal hemorrhage and why is it dangerous?
Subgaleal hemorrhage is bleeding into the subaponeurotic space, often after vacuum delivery. It can cause massive blood loss, shock, and is a neonatal emergency.
What are red flag signs requiring urgent referral in abnormal head size or shape?
Red flags include rapidly increasing head circumference, bulging fontanelle, seizures, vomiting, developmental regression, suspected craniosynostosis, signs of raised intracranial pressure, or suspected abusive head trauma.
MCQ Test - Abnormal Head Size and Shape in Pediatrics Microcephaly Macrocephaly Craniosynostosis Guide
Progress:
0/15
Time: 00:00
Test Results
0%
0/15
0
Correct Answers
0
Wrong Answers
00:00
Time Taken
0
Skipped