Medical Disclaimer: This is educational content only, not medical advice. Consult a licensed healthcare provider for diagnosis/treatment. Information based on sources like WHO/CDC guidelines (last reviewed: 2026-02-13).
This article is being expanded for more depth. Check back soon!
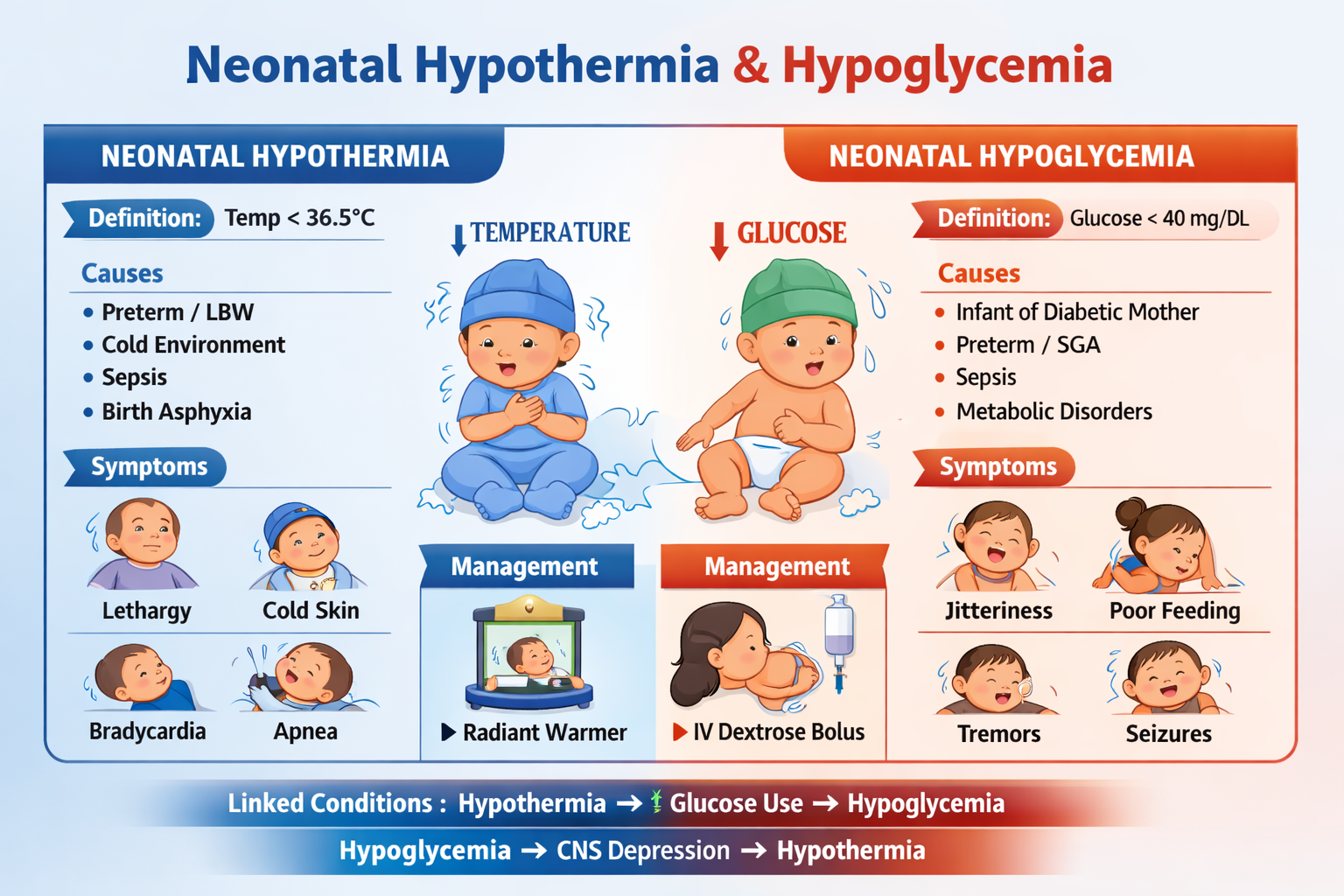
Neonatal Hypothermia and Hypoglycemia Diagnosis Causes Management Guide
Frequently Asked Questions
What is neonatal hypothermia?
Neonatal hypothermia is defined as a newborn core body temperature below 36.5°C. It occurs because neonates have immature thermoregulation, large surface area, thin skin, and limited fat stores.
How is neonatal hypothermia classified by WHO?
WHO classifies neonatal hypothermia as mild (36.0–36.4°C), moderate (32.0–35.9°C), and severe (<32°C).
Why are newborns at high risk of hypothermia?
Newborns lose heat rapidly due to large surface area-to-weight ratio, minimal subcutaneous fat, inability to shiver effectively, and reliance on brown fat metabolism for heat production.
What are the major causes of neonatal hypothermia?
Major causes include cold delivery environments, delayed drying and wrapping, prematurity, low birth weight, neonatal sepsis, birth asphyxia, and inadequate warming during transport.
What are the clinical signs of neonatal hypothermia?
Signs include cold skin, lethargy, poor feeding, tachypnea, bradycardia, apnea, metabolic acidosis, hypoglycemia, and increased risk of sepsis.
What is neonatal hypoglycemia?
Neonatal hypoglycemia refers to low blood glucose levels in newborns, commonly defined as <45 mg/dL after 24 hours of life, which can cause neuroglycopenia and seizures if untreated.
Which newborns are at highest risk for hypoglycemia?
High-risk groups include infants of diabetic mothers, preterm babies, small for gestational age infants, large for gestational age infants, babies with sepsis, hypothermia, or birth asphyxia.
What are the symptoms of neonatal hypoglycemia?
Symptoms include jitteriness, tremors, poor feeding, lethargy, apnea, hypotonia, cyanosis, and seizures in severe or prolonged cases.
How are neonatal hypothermia and hypoglycemia related?
Hypothermia increases glucose consumption due to cold stress, leading to hypoglycemia. Hypoglycemia causes CNS depression, reducing thermoregulation and worsening hypothermia.
What is the first-line treatment for symptomatic neonatal hypoglycemia?
Symptomatic or severe hypoglycemia is treated immediately with 10% dextrose bolus 2 mL/kg IV, followed by continuous glucose infusion with close monitoring.
How is neonatal hypothermia managed?
Management includes immediate drying, skin-to-skin warming for mild cases, radiant warmer or incubator care for moderate cases, controlled rewarming in NICU for severe cases, and treating underlying causes like sepsis.
What complications can occur if neonatal hypothermia is untreated?
Untreated hypothermia can cause hypoglycemia, metabolic acidosis, respiratory failure, persistent pulmonary hypertension, shock, and increased neonatal mortality.
What complications can occur if neonatal hypoglycemia is untreated?
Untreated hypoglycemia can lead to seizures, permanent brain injury, developmental delay, cerebral palsy, and increased risk of death.
What investigations are important in recurrent neonatal hypoglycemia?
Key investigations include plasma glucose confirmation, insulin levels, ketones, cortisol, growth hormone, metabolic screening, and evaluation for congenital hyperinsulinism or endocrine disorders.
How can neonatal hypothermia and hypoglycemia be prevented?
Prevention includes maintaining the warm chain at birth, early drying and wrapping, kangaroo mother care, early breastfeeding, screening high-risk newborns, and ensuring proper NICU thermal support.
MCQ Test - Neonatal Hypothermia and Hypoglycemia Diagnosis Causes Management Guide
Progress:
0/15
Time: 00:00
Test Results
0%
0/15
0
Correct Answers
0
Wrong Answers
00:00
Time Taken
0
Skipped