Medical Disclaimer: This is educational content only, not medical advice. Consult a licensed healthcare provider for diagnosis/treatment. Information based on sources like WHO/CDC guidelines (last reviewed: 2026-02-13).
This article is being expanded for more depth. Check back soon!
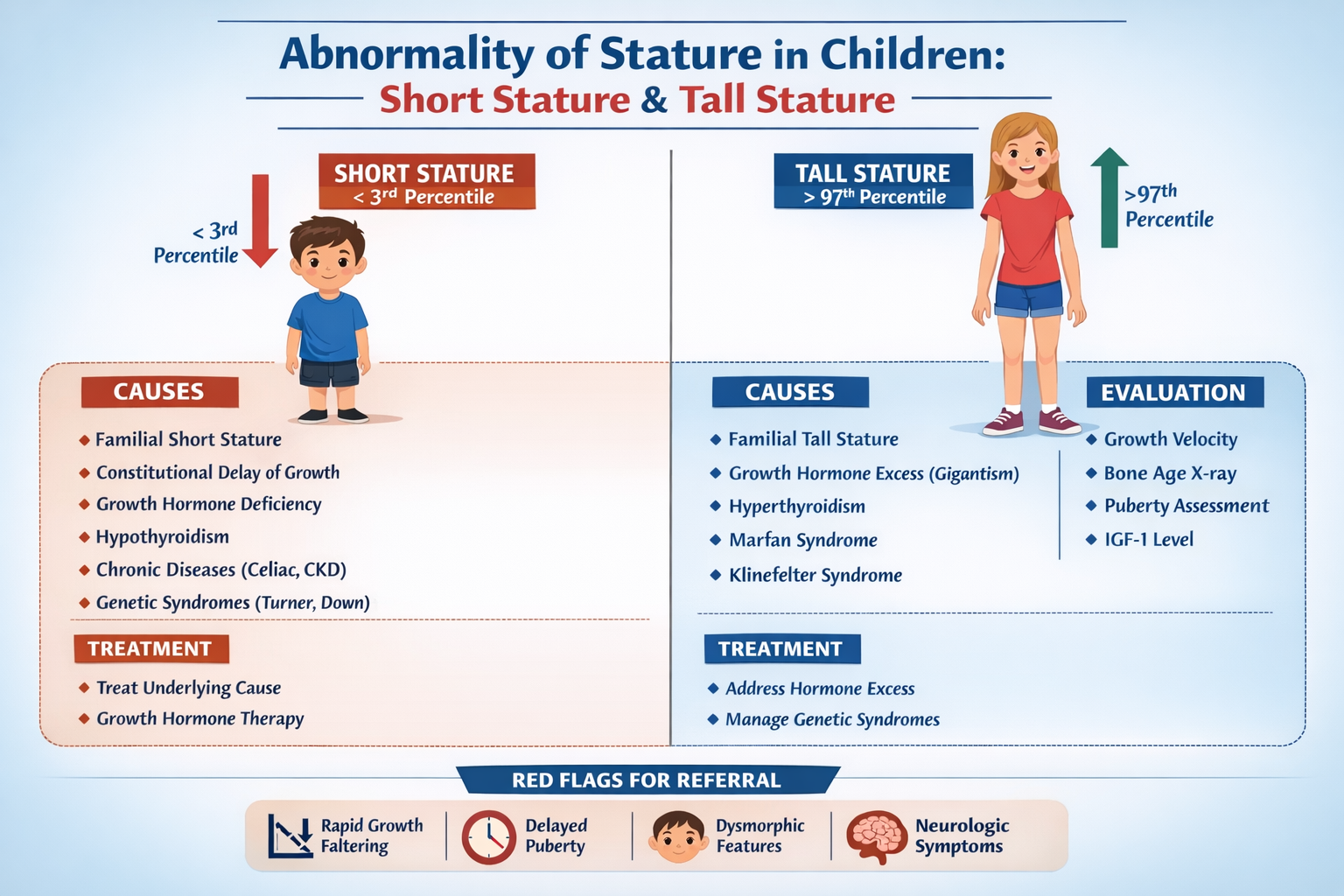
Abnormality of Stature in Children: Short Stature, Tall Stature Causes and Management
Frequently Asked Questions
What is meant by abnormality of stature in children?
Abnormality of stature refers to deviation of a child’s height from the normal range for age and sex. It includes short stature (height below the 3rd percentile or < –2 SD) and tall stature (height above the 97th percentile or > +2 SD).
How is short stature defined clinically?
Short stature is defined as height less than the 3rd percentile or more than 2 standard deviations below the mean for age and sex, or when growth velocity is significantly reduced.
What is the most common cause of short stature worldwide?
The most common cause of short stature worldwide is malnutrition, which leads to impaired linear growth due to inadequate caloric and protein intake.
What are the normal variants of short stature?
Normal variants include familial short stature (genetic short parents, normal bone age) and constitutional delay of growth and puberty (delayed bone age, late puberty but normal final height).
How can familial short stature be distinguished from constitutional delay?
Familial short stature has normal bone age equal to chronological age, while constitutional delay shows delayed bone age and delayed puberty with eventual catch-up growth.
What endocrine disorders commonly cause short stature?
Endocrine causes include growth hormone deficiency, hypothyroidism, Cushing syndrome, and poorly controlled diabetes mellitus.
What are clinical features suggestive of growth hormone deficiency?
Features include poor growth velocity, delayed bone age, increased truncal fat, immature facial appearance, and sometimes hypoglycemia in infancy.
Why does hypothyroidism cause growth failure?
Thyroid hormone is essential for growth plate maturation. Deficiency leads to reduced growth velocity, delayed skeletal maturation, and short stature.
How do chronic systemic diseases affect growth?
Chronic diseases like renal failure, congenital heart disease, tuberculosis, and inflammatory bowel disease impair growth, typically with weight loss occurring before height impairment.
What genetic syndromes are associated with short stature?
Turner syndrome, Down syndrome, Noonan syndrome, and skeletal dysplasias such as achondroplasia are important genetic causes.
When should Turner syndrome be suspected in a girl with short stature?
Turner syndrome should be suspected when short stature is associated with webbed neck, shield chest, widely spaced nipples, delayed puberty, or primary amenorrhea.
What is bone age and why is it important in growth evaluation?
Bone age is assessed by X-ray of the left hand and wrist. It helps differentiate normal variants (familial short stature) from endocrine disorders or constitutional delay.
What does delayed bone age indicate?
Delayed bone age suggests constitutional delay of growth and puberty, growth hormone deficiency, hypothyroidism, or chronic systemic illness.
What does advanced bone age indicate?
Advanced bone age is typically seen in precocious puberty, hyperthyroidism, congenital adrenal hyperplasia, or androgen excess states.
What baseline investigations are recommended in short stature?
Baseline workup includes CBC, ESR/CRP, renal and liver function tests, thyroid function tests, celiac serology, and bone age assessment.
What is tall stature in pediatrics?
Tall stature is defined as height above the 97th percentile or more than +2 standard deviations above the mean for age and sex.
What are common causes of tall stature?
Causes include familial tall stature, growth hormone excess (gigantism), hyperthyroidism, precocious puberty, and genetic syndromes such as Marfan syndrome and Klinefelter syndrome.
How does gigantism present clinically?
Gigantism presents with excessive growth velocity, coarse facial features, enlarged hands and feet, elevated IGF-1, and often pituitary adenoma symptoms such as headache or visual defects.
What are the red flags requiring urgent referral in abnormal stature?
Red flags include rapid crossing of growth percentiles, very low growth velocity, dysmorphic features, delayed or absent puberty, neurological symptoms, and suspicion of systemic disease.
When is growth hormone therapy indicated?
Growth hormone therapy is indicated in GH deficiency, Turner syndrome, chronic renal failure, Prader-Willi syndrome, children born small for gestational age without catch-up growth, and selected idiopathic short stature cases.
What are important adverse effects of growth hormone therapy?
Adverse effects include intracranial hypertension, slipped capital femoral epiphysis, worsening scoliosis, hyperglycemia, and edema, requiring careful monitoring.
How is abnormal stature best managed overall?
Management depends on identifying the underlying cause, addressing nutrition and chronic illness, treating endocrine disorders, considering growth hormone therapy when appropriate, and monitoring growth velocity and pubertal development.
MCQ Test - Abnormality of Stature in Children: Short Stature, Tall Stature Causes and Management
Progress:
0/15
Time: 00:00
Test Results
0%
0/15
0
Correct Answers
0
Wrong Answers
00:00
Time Taken
0
Skipped