Medical Disclaimer: This is educational content only, not medical advice. Consult a licensed healthcare provider for diagnosis/treatment. Information based on sources like WHO/CDC guidelines (last reviewed: 2026-02-13).
This article is being expanded for more depth. Check back soon!
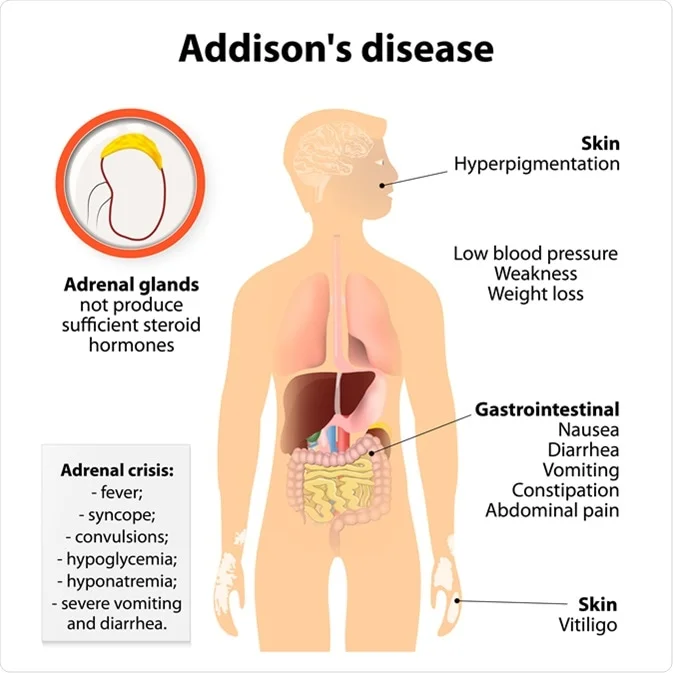
Addison’s Disease Comprehensive Clinical Guide Diagnosis Causes and Management
Frequently Asked Questions
What is Addison’s disease?
Addison’s disease is primary adrenal insufficiency caused by destruction or dysfunction of the adrenal cortex, resulting in deficiency of cortisol, aldosterone, and adrenal androgens.
How is Addison’s disease different from secondary adrenal insufficiency?
Addison’s disease involves adrenal gland failure with high ACTH and hyperkalemia, while secondary adrenal insufficiency is due to pituitary or hypothalamic causes with normal aldosterone and no hyperkalemia.
What is the most common cause of Addison’s disease?
Autoimmune adrenalitis is the most common cause in developed countries, while tuberculosis is the most common cause worldwide.
Why does hyperpigmentation occur in Addison’s disease?
Loss of cortisol feedback causes elevated ACTH, which increases melanocyte-stimulating hormone activity, leading to hyperpigmentation.
What are the hallmark electrolyte abnormalities in Addison’s disease?
Hyponatremia and hyperkalemia due to aldosterone deficiency are hallmark findings.
What is the gold standard diagnostic test for Addison’s disease?
The ACTH (cosyntropin) stimulation test is the gold standard for diagnosis.
What is Addisonian crisis?
Addisonian crisis is a life-threatening emergency characterized by hypotension, shock, hypoglycemia, vomiting, and electrolyte imbalance.
What is the immediate treatment for Addisonian crisis?
Immediate IV hydrocortisone, aggressive IV normal saline with dextrose, correction of electrolytes, and treatment of the precipitating cause.
What medications are used for long-term treatment of Addison’s disease?
Lifelong glucocorticoid replacement with hydrocortisone and mineralocorticoid replacement with fludrocortisone.
Why is stress-dose steroid therapy important?
During illness, surgery, or trauma, steroid requirements increase; failure to increase doses can precipitate adrenal crisis.
Can Addison’s disease be cured?
Addison’s disease cannot be cured, but it can be effectively managed with lifelong hormone replacement therapy.
Which autoimmune conditions are commonly associated with Addison’s disease?
Type 1 diabetes, autoimmune thyroid disease, pernicious anemia, and vitiligo as part of autoimmune polyglandular syndrome type 2.
Why do women with Addison’s disease lose axillary and pubic hair?
Due to deficiency of adrenal androgens, which contribute to secondary sexual hair in women.
What patient education is essential in Addison’s disease?
Never stopping steroids abruptly, carrying a medical alert ID, using stress dosing during illness, and having emergency injectable hydrocortisone.
What is the prognosis of Addison’s disease?
With proper treatment, compliance, and patient education, the prognosis is excellent.
MCQ Test - Addison’s Disease Comprehensive Clinical Guide Diagnosis Causes and Management
Progress:
0/15
Time: 00:00
Test Results
0%
0/15
0
Correct Answers
0
Wrong Answers
00:00
Time Taken
0
Skipped