Medical Disclaimer: This is educational content only, not medical advice. Consult a licensed healthcare provider for diagnosis/treatment. Information based on sources like WHO/CDC guidelines (last reviewed: 2026-02-13).
This article is being expanded for more depth. Check back soon!
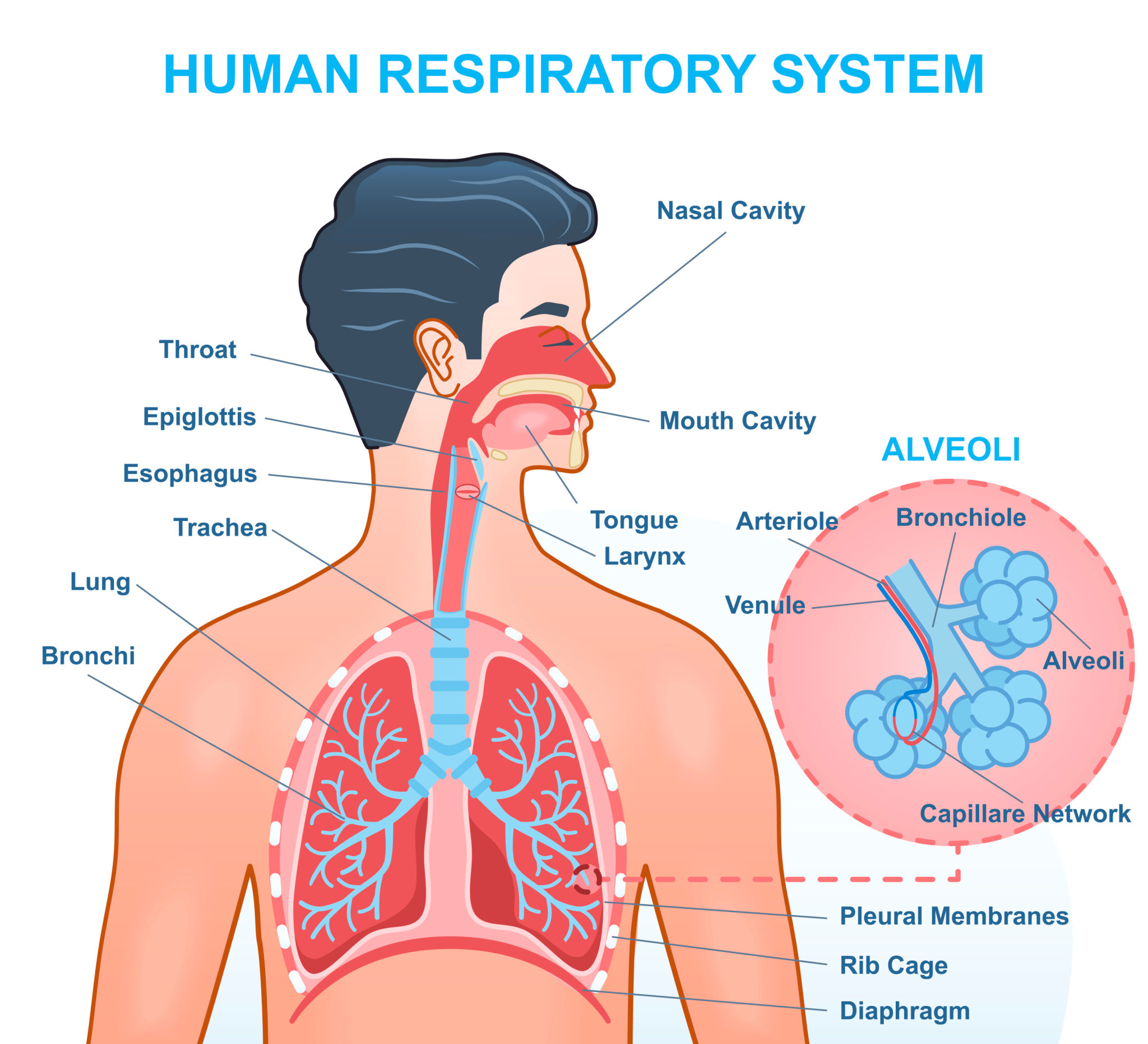
Respiratory System Physiology Complete Guide for Medical Students
Frequently Asked Questions
What is the primary function of the respiratory system?
The primary function of the respiratory system is gas exchange, which involves uptake of oxygen into the blood and elimination of carbon dioxide from the body. It also plays a crucial role in acid–base balance, phonation, defense mechanisms, and metabolic functions.
What is the difference between ventilation and respiration?
Ventilation refers to the mechanical movement of air into and out of the lungs, while respiration includes ventilation, diffusion of gases across the alveolar membrane, transport of gases in blood, and cellular utilization of oxygen.
What determines alveolar ventilation?
Alveolar ventilation is determined by tidal volume, respiratory rate, and dead space. It is calculated as (tidal volume minus dead space) multiplied by respiratory rate and directly influences arterial carbon dioxide levels.
Why is surfactant important in lung physiology?
Pulmonary surfactant reduces surface tension within alveoli, preventing alveolar collapse during expiration, increasing lung compliance, and reducing the work of breathing. It is produced by type II pneumocytes.
What is the ventilation perfusion ratio and why is it important?
The ventilation perfusion ratio is the ratio of alveolar ventilation to pulmonary blood flow. A normal value is about 0.8. Matching of ventilation and perfusion is essential for efficient gas exchange, and mismatch leads to hypoxemia.
What causes hypoxemia that does not improve with oxygen therapy?
Physiological shunt is the main cause of hypoxemia that does not correct with oxygen therapy, as blood bypasses ventilated alveoli, commonly seen in pneumonia and pulmonary edema.
What factors shift the oxyhemoglobin dissociation curve to the right?
Increased carbon dioxide, increased hydrogen ion concentration, increased temperature, and increased 2,3-BPG shift the curve to the right, facilitating oxygen unloading to tissues.
Which chemoreceptors are most sensitive to carbon dioxide changes?
Central chemoreceptors located in the medulla are most sensitive to changes in carbon dioxide via changes in cerebrospinal fluid pH and provide the strongest drive for respiration.
What is the physiological basis of respiratory acidosis?
Respiratory acidosis occurs due to hypoventilation leading to carbon dioxide retention, increased PaCO₂, and a fall in blood pH. Renal compensation occurs by increased bicarbonate reabsorption.
Why does emphysema cause difficulty in expiration?
Emphysema causes destruction of elastic tissue in the lungs, leading to loss of elastic recoil. This results in airway collapse during expiration and air trapping.
MCQ Test - Respiratory System Physiology Complete Guide for Medical Students
Progress:
0/15
Time: 00:00
Test Results
0%
0/15
0
Correct Answers
0
Wrong Answers
00:00
Time Taken
0
Skipped