Medical Disclaimer: This is educational content only, not medical advice. Consult a licensed healthcare provider for diagnosis/treatment. Information based on sources like WHO/CDC guidelines (last reviewed: 2026-02-13).
This article is being expanded for more depth. Check back soon!
Rheumatic Heart Disease Clinical Features Diagnosis Management and Prevention
Frequently Asked Questions
What is rheumatic heart disease?
Rheumatic heart disease is a chronic valvular heart condition caused by immune-mediated damage following acute rheumatic fever, which occurs after untreated or inadequately treated Group A streptococcal throat infection.
Which heart valves are most commonly affected in rheumatic heart disease?
The mitral valve is most commonly affected, followed by the aortic valve. Tricuspid involvement is usually secondary, and pulmonary valve involvement is rare.
How does acute rheumatic fever lead to rheumatic heart disease?
Acute rheumatic fever causes an autoimmune reaction due to molecular mimicry between streptococcal antigens and cardiac tissue, leading to inflammation, fibrosis, and permanent valvular damage.
What are the common symptoms of rheumatic mitral stenosis?
Common symptoms include exertional dyspnea, orthopnea, paroxysmal nocturnal dyspnea, hemoptysis, palpitations due to atrial fibrillation, and thromboembolic events such as stroke.
Why is atrial fibrillation common in rheumatic heart disease?
Left atrial enlargement due to mitral stenosis or regurgitation predisposes to atrial fibrillation, increasing the risk of thromboembolism.
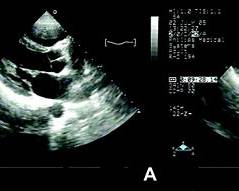
What investigation confirms the diagnosis of rheumatic heart disease?
Echocardiography is the gold standard investigation as it defines valve morphology, severity of stenosis or regurgitation, chamber sizes, pulmonary pressures, and complications like atrial thrombus.
What is the role of secondary prophylaxis in rheumatic heart disease?
Secondary prophylaxis with long-acting benzathine penicillin prevents recurrent streptococcal infections and recurrent rheumatic fever, thereby slowing progression of valvular damage.
How long should secondary penicillin prophylaxis be continued?
Duration depends on severity: at least 5 years or until age 21 without carditis, 10 years or until age 21 with carditis, and often lifelong in patients with residual valvular disease.
When is balloon mitral valvotomy indicated in rheumatic heart disease?
It is indicated in symptomatic severe rheumatic mitral stenosis with favorable valve anatomy and absence of left atrial thrombus or significant mitral regurgitation.
Why are DOACs not preferred in rheumatic mitral stenosis with atrial fibrillation?
Warfarin is preferred because clinical trials have shown inferior protection with direct oral anticoagulants in rheumatic mitral stenosis.
What are the common complications of rheumatic heart disease?
Complications include atrial fibrillation, thromboembolism, infective endocarditis, pulmonary hypertension, heart failure, stroke, and sudden cardiac death.
How does pregnancy affect rheumatic heart disease?
Pregnancy increases blood volume and heart rate, which can precipitate pulmonary edema and heart failure, especially in mitral stenosis.
What is Ortner syndrome in rheumatic heart disease?
Ortner syndrome refers to hoarseness of voice due to compression of the left recurrent laryngeal nerve by an enlarged left atrium in severe mitral stenosis.
When is valve surgery indicated in rheumatic heart disease?
Valve surgery is indicated in severe symptomatic valvular disease, presence of left ventricular dysfunction, or when percutaneous intervention is not suitable.
How can rheumatic heart disease be prevented?
Prevention includes early treatment of streptococcal pharyngitis, long-term secondary prophylaxis after rheumatic fever, improved living conditions, and access to primary healthcare.
MCQ Test - Rheumatic Heart Disease Clinical Features Diagnosis Management and Prevention
Progress:
0/15
Time: 00:00
Test Results
0%
0/15
0
Correct Answers
0
Wrong Answers
00:00
Time Taken
0
Skipped