Medical Disclaimer: This is educational content only, not medical advice. Consult a licensed healthcare provider for diagnosis/treatment. Information based on sources like WHO/CDC guidelines (last reviewed: 2026-02-13).
Second Heart Sound S2 Clinical Features Physiology Splitting and Causes
Frequently Asked Questions
What is the second heart sound S2?
The second heart sound S2 is produced by the closure of the semilunar valves, specifically the aortic valve (A2) and pulmonary valve (P2), marking the end of ventricular systole and the beginning of diastole.
Which valves are responsible for S2?
S2 is caused by closure of the aortic valve (A2) and the pulmonary valve (P2).
Where is S2 best heard on auscultation?
S2 is best heard at the base of the heart, with A2 at the right second intercostal space and P2 at the left second intercostal space.
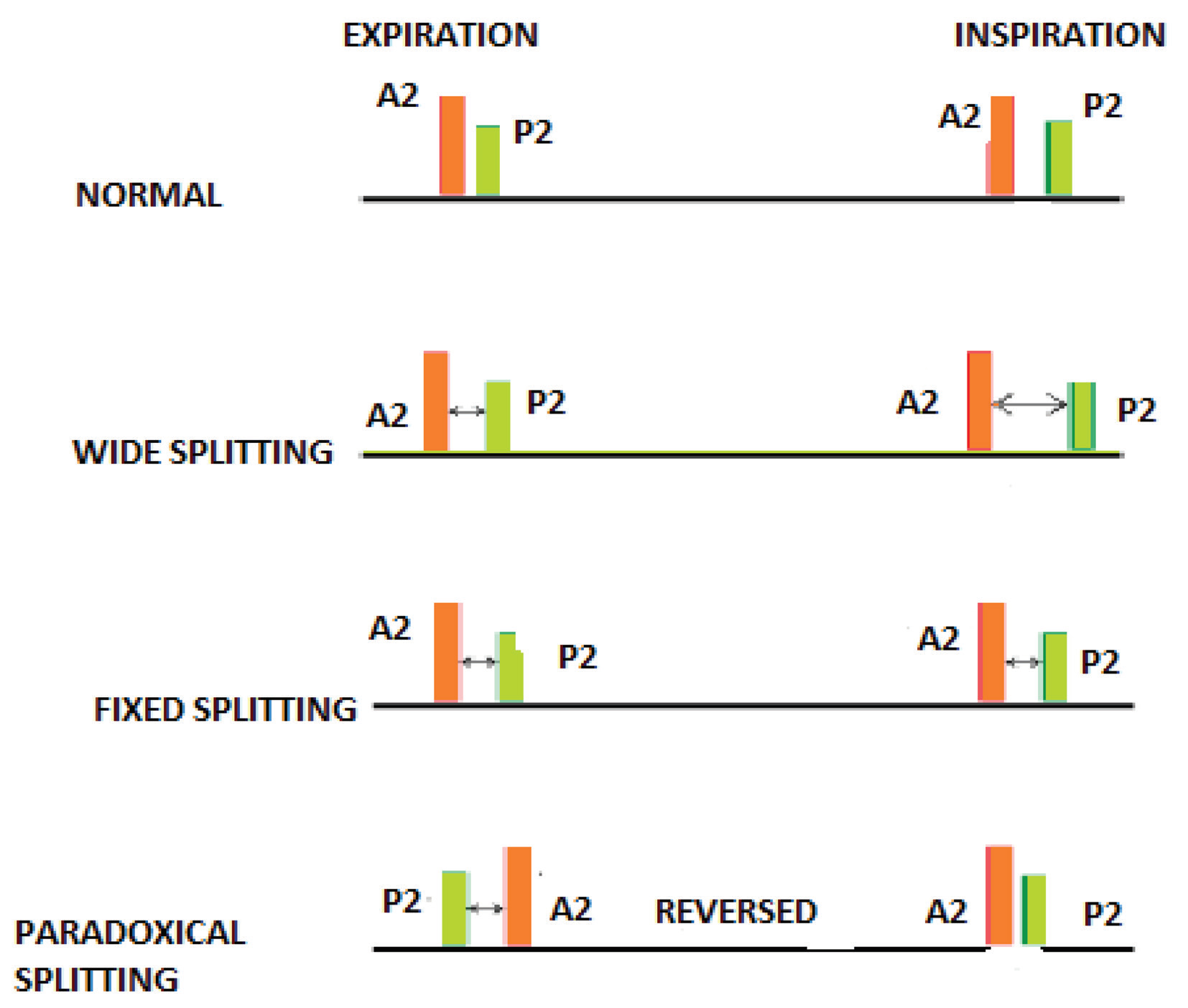
What is physiological splitting of S2?
Physiological splitting of S2 refers to normal separation of A2 and P2 during inspiration due to delayed right ventricular emptying and delayed P2.
What causes wide splitting of S2?
Wide splitting of S2 occurs due to delayed P2 and is seen in conditions such as right bundle branch block, pulmonary stenosis, and pulmonary embolism.
What is fixed splitting of S2 and its significance?
Fixed splitting of S2 is a constant split during both inspiration and expiration and is classically associated with atrial septal defect.
What is paradoxical splitting of S2?
Paradoxical splitting of S2 occurs when the split is heard during expiration and disappears during inspiration, usually due to delayed A2 as seen in left bundle branch block or severe aortic stenosis.
What does a loud A2 indicate?
A loud A2 usually indicates systemic hypertension due to increased force of aortic valve closure.
What conditions cause a soft or absent A2?
A soft or absent A2 is seen in severe aortic stenosis and severe aortic regurgitation.
What is the clinical significance of a loud P2?
A loud or accentuated P2 is an important clinical sign of pulmonary hypertension.
What causes a soft or absent P2?
A soft or absent P2 is commonly caused by pulmonary stenosis due to reduced pulmonary valve closure force.
What does a single S2 suggest?
A single S2 may suggest severe aortic stenosis or severe pulmonary stenosis where one component is absent.
Which stethoscope component is best for hearing S2?
S2 is a high-frequency sound and is best heard using the diaphragm of the stethoscope.
How does S2 help in diagnosing pulmonary hypertension?
An accentuated and palpable P2 on auscultation is an early and reliable marker of pulmonary hypertension.
Why does S2 normally split during inspiration?
During inspiration, increased venous return delays right ventricular emptying, resulting in delayed pulmonary valve closure and splitting of S2.
MCQ Test - Second Heart Sound S2 Clinical Features Physiology Splitting and Causes
Progress:
0/0
Time: 00:00
No MCQs available for this article.