Medical Disclaimer: This is educational content only, not medical advice. Consult a licensed healthcare provider for diagnosis/treatment. Information based on sources like WHO/CDC guidelines (last reviewed: 2026-02-13).
First Heart Sound S1 and Jugular Venous Pulse JVP Clinical Examination Guide
Frequently Asked Questions
What is the first heart sound (S1)?
The first heart sound (S1) is produced by the closure of the atrioventricular valves—mitral (M1) and tricuspid (T1)—at the beginning of ventricular systole during the isovolumetric contraction phase.
Which valve component contributes most to S1?
The mitral component (M1) contributes most to S1 and is best heard at the cardiac apex.
What factors make S1 loud?
A loud S1 is caused by a short PR interval, mobile mitral valve leaflets (as in mitral stenosis), hyperdynamic circulation (fever, anemia, thyrotoxicosis), and thin chest wall.
What causes a soft S1?
A soft S1 occurs due to long PR interval, mitral regurgitation, calcified mitral valve, left ventricular failure, obesity, or emphysema.
Why is S1 variable in atrial fibrillation?
In atrial fibrillation, the PR interval varies beat to beat, leading to variable timing of AV valve closure and hence variable intensity of S1.
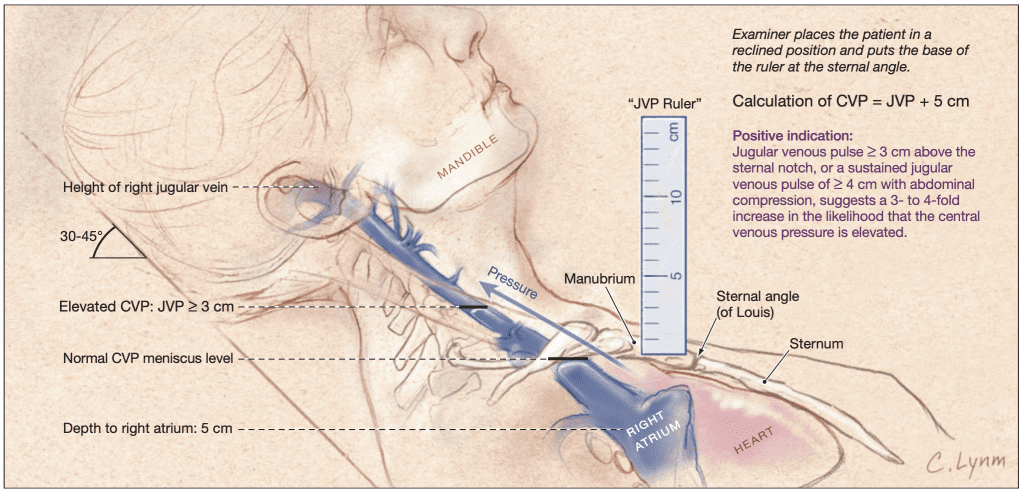
What is the jugular venous pulse (JVP)?
The jugular venous pulse is the visible pulsation of the internal jugular vein reflecting right atrial pressure and right heart hemodynamics.
Why is the internal jugular vein preferred for JVP assessment?
The internal jugular vein has a direct connection to the right atrium, lacks valves, and accurately reflects central venous pressure.
What are the normal components of the JVP waveform?
The normal JVP waveform consists of a wave (atrial contraction), c wave (tricuspid bulging), x descent (atrial relaxation), v wave (venous filling), and y descent (ventricular filling).
What does a raised JVP indicate?
A raised JVP indicates elevated right atrial pressure and is seen in right heart failure, tricuspid valve disease, constrictive pericarditis, cardiac tamponade, pulmonary hypertension, and fluid overload.
What causes absent a waves in JVP?
Absent a waves are seen in atrial fibrillation due to the absence of organized atrial contraction.
What are cannon a waves and when are they seen?
Cannon a waves are large intermittent a waves caused by atrial contraction against a closed tricuspid valve, seen in complete heart block and other AV dissociation states.
Which condition causes prominent v waves in JVP?
Prominent v waves are characteristic of tricuspid regurgitation due to systolic backflow of blood into the right atrium.
What is Kussmaul’s sign?
Kussmaul’s sign is a paradoxical rise in JVP during inspiration, seen in constrictive pericarditis, restrictive cardiomyopathy, and right ventricular infarction.
How does JVP differ in cardiac tamponade?
In cardiac tamponade, JVP is raised with a prominent x descent and an absent y descent due to impaired ventricular filling.
What is the clinical importance of examining S1 and JVP together?
Combined assessment of S1 and JVP helps in diagnosing valvular heart disease, arrhythmias, right heart failure, and pericardial disorders at the bedside.
MCQ Test - First Heart Sound S1 and Jugular Venous Pulse JVP Clinical Examination Guide
Progress:
0/15
Time: 00:00
Test Results
0%
0/15
0
Correct Answers
0
Wrong Answers
00:00
Time Taken
0
Skipped