Medical Disclaimer: This is educational content only, not medical advice. Consult a licensed healthcare provider for diagnosis/treatment. Information based on sources like WHO/CDC guidelines (last reviewed: 2026-02-13).
Tricuspid and Pulmonary Valve Murmurs Explained TS TR PS PR Clinical Guide
Frequently Asked Questions
What are right-sided heart murmurs?
Right-sided heart murmurs originate from the tricuspid or pulmonary valves and include tricuspid stenosis, tricuspid regurgitation, pulmonary stenosis, and pulmonary regurgitation. They characteristically become louder with inspiration due to increased venous return to the right heart.
Which murmurs increase in intensity with inspiration?
Tricuspid regurgitation, tricuspid stenosis, pulmonary stenosis, and pulmonary regurgitation typically increase with inspiration. This phenomenon is known as Carvallo sign and helps differentiate right-sided from left-sided murmurs.
What is the classic murmur of tricuspid regurgitation?
Tricuspid regurgitation produces a holosystolic murmur best heard at the left lower sternal border that becomes louder with inspiration and may be associated with prominent V waves in the jugular venous pulse.
How does tricuspid stenosis murmur differ from mitral stenosis murmur?
Tricuspid stenosis murmur is a low-pitched mid-diastolic murmur heard best at the left lower sternal border and increases with inspiration, whereas mitral stenosis is best heard at the apex and is louder during expiration.
What causes pulmonary stenosis murmur?
Pulmonary stenosis murmur is caused by obstruction to right ventricular outflow, producing an ejection systolic crescendo–decrescendo murmur at the left upper sternal border, often with an ejection click.
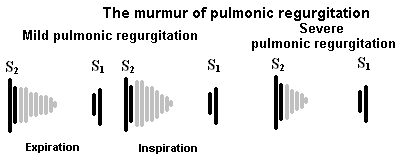
What is Graham Steell murmur?
Graham Steell murmur is a high-pitched early diastolic murmur of pulmonary regurgitation caused by severe pulmonary hypertension and is best heard at the left upper sternal border.
Which murmur is most commonly associated with intravenous drug use?
Tricuspid regurgitation is most commonly associated with intravenous drug use due to infective endocarditis affecting the tricuspid valve.
What jugular venous pulse finding is typical of tricuspid regurgitation?
Tricuspid regurgitation is associated with prominent V waves in the jugular venous pulse due to systolic backflow of blood into the right atrium.
What happens to presystolic accentuation in atrial fibrillation?
Presystolic accentuation disappears in atrial fibrillation because it depends on atrial contraction, which is absent in atrial fibrillation.
What is the definitive treatment for severe pulmonary regurgitation with right ventricular dilation?
Pulmonary valve replacement, either surgical or transcatheter, is the definitive treatment for severe pulmonary regurgitation associated with right ventricular dilation or dysfunction.
Which valve lesion is commonly associated with carcinoid syndrome?
Carcinoid syndrome most commonly affects the tricuspid valve, leading to tricuspid regurgitation due to fibrotic plaque deposition.
How can tricuspid regurgitation be differentiated from ventricular septal defect on auscultation?
Tricuspid regurgitation murmur increases with inspiration, whereas the murmur of ventricular septal defect does not show inspiratory augmentation.
Which murmur is common after repair of Tetralogy of Fallot?
Pulmonary regurgitation is common after Tetralogy of Fallot repair and presents as an early diastolic decrescendo murmur at the left upper sternal border.
What is the most common cause of tricuspid stenosis worldwide?
Rheumatic heart disease is the most common cause of tricuspid stenosis worldwide, often occurring in association with mitral stenosis.
Why are diastolic murmurs considered pathological?
Diastolic murmurs almost always indicate structural heart disease because normal blood flow during diastole does not usually produce audible turbulence.
MCQ Test - Tricuspid and Pulmonary Valve Murmurs Explained TS TR PS PR Clinical Guide
Progress:
0/15
Time: 00:00
Test Results
0%
0/15
0
Correct Answers
0
Wrong Answers
00:00
Time Taken
0
Skipped