Medical Disclaimer: This is educational content only, not medical advice. Consult a licensed healthcare provider for diagnosis/treatment. Information based on sources like WHO/CDC guidelines (last reviewed: 2026-02-13).
This article is being expanded for more depth. Check back soon!
First Heart Sound S1 S3 S4 Atrial Myxoma Papillary Fibroelastoma Tuberculous Pericarditis Constrictive Pericarditis Complete Guide
Frequently Asked Questions
What is the first heart sound S1?
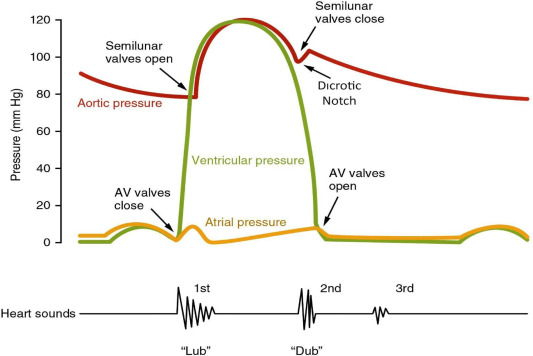
The first heart sound S1 is produced by closure of the mitral and tricuspid valves at the onset of ventricular systole. It marks the beginning of systole and is best heard at the apex.
What causes variation in intensity of S1?
Variation in S1 intensity depends on valve mobility, PR interval duration, ventricular contractility, and rhythm irregularity such as atrial fibrillation.
What is the clinical significance of the S3 heart sound?
S3 indicates rapid ventricular filling and is physiological in children and young adults but pathological in older adults, commonly suggesting heart failure or volume overload.
Why is S4 called an atrial gallop?
S4 is caused by atrial contraction against a stiff, non-compliant ventricle, hence termed an atrial gallop and is associated with diastolic dysfunction.
In which condition is S4 always absent?
S4 is absent in atrial fibrillation because it requires effective atrial contraction.
What is atrial myxoma?
Atrial myxoma is the most common primary benign cardiac tumor, usually arising from the left atrium near the interatrial septum.
What are the classical clinical features of atrial myxoma?
The classical triad includes obstructive symptoms, embolic events, and constitutional symptoms such as fever and weight loss due to IL-6 secretion.
What is a tumor plop?
A tumor plop is an early diastolic sound caused by sudden movement of an atrial myxoma through the mitral valve.
What is papillary fibroelastoma?
Papillary fibroelastoma is a benign cardiac tumor commonly arising from heart valves and is highly emboligenic despite its small size.
Which investigation is best for diagnosing papillary fibroelastoma?
Transesophageal echocardiography is the investigation of choice due to its high sensitivity for small valvular lesions.
What is tuberculous pericarditis?
Tuberculous pericarditis is an infection of the pericardium caused by Mycobacterium tuberculosis, common in TB-endemic regions.
What are the stages of tuberculous pericarditis?
The stages include dry fibrinous, effusive, absorptive, and constrictive stages.
What is the role of corticosteroids in tuberculous pericarditis?
Corticosteroids reduce inflammation and decrease the risk of progression to constrictive pericarditis when used along with anti-tubercular therapy.
What is constrictive pericarditis?
Constrictive pericarditis is a condition where the pericardium becomes thickened and fibrotic, restricting diastolic filling of the heart.
What is the most common cause of constrictive pericarditis worldwide?
Tuberculous pericarditis is the most common cause of constrictive pericarditis worldwide.
What is a pericardial knock?
A pericardial knock is an early diastolic sound caused by abrupt cessation of ventricular filling in constrictive pericarditis.
How is constrictive pericarditis differentiated from restrictive cardiomyopathy?
Constrictive pericarditis is differentiated by presence of pericardial thickening, pericardial knock, and ventricular interdependence on imaging and hemodynamic studies.
What is the definitive treatment for constrictive pericarditis?
The definitive treatment is surgical pericardiectomy.
What prognosis does S3 indicate in heart failure?
Presence of S3 in heart failure indicates elevated filling pressures and is associated with poor prognosis.
Which heart sound best indicates diastolic dysfunction?
S4 heart sound best indicates diastolic dysfunction due to reduced ventricular compliance.
MCQ Test - First Heart Sound S1 S3 S4 Atrial Myxoma Papillary Fibroelastoma Tuberculous Pericarditis Constrictive Pericarditis Complete Guide
Progress:
0/0
Time: 00:00
No MCQs available for this article.