Medical Disclaimer: This is educational content only, not medical advice. Consult a licensed healthcare provider for diagnosis/treatment. Information based on sources like WHO/CDC guidelines (last reviewed: 2026-02-13).
This article is being expanded for more depth. Check back soon!
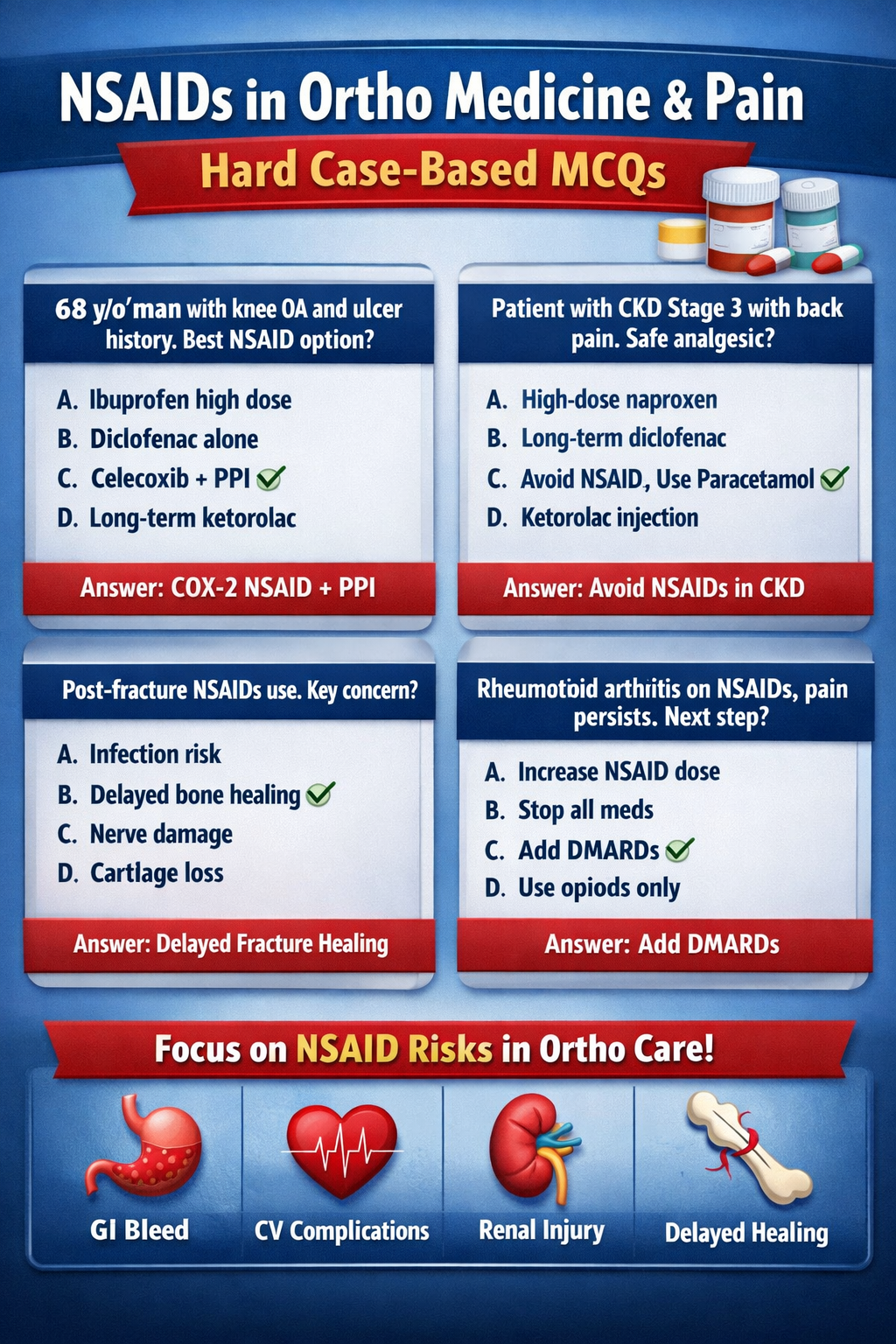
NSAIDs Uses and Risks in Orthopedic Medicine and Pain Management Guide
Frequently Asked Questions
What are NSAIDs and how do they work in pain management?
NSAIDs (Non-Steroidal Anti-Inflammatory Drugs) reduce pain, inflammation, and fever by inhibiting COX enzymes and decreasing prostaglandin production.
What are the main uses of NSAIDs in orthopedic medicine?
NSAIDs are used for osteoarthritis, rheumatoid arthritis, acute musculoskeletal injuries, post-operative pain, tendinitis, bursitis, and sports-related inflammation.
Why are NSAIDs effective for inflammatory pain but not neuropathic pain?
NSAIDs target inflammatory pathways, while neuropathic pain arises from nerve damage and responds better to drugs like gabapentin or pregabalin.
What is the biggest gastrointestinal risk of NSAIDs?
NSAIDs can cause gastritis, peptic ulcers, gastrointestinal bleeding, and perforation due to reduced gastric mucosal protection.
How do NSAIDs affect kidney function?
NSAIDs reduce renal prostaglandins, leading to decreased renal blood flow, fluid retention, electrolyte imbalance, and possible acute kidney injury.
Why are NSAIDs risky in elderly patients?
Elderly patients have higher risk of GI bleeding, kidney injury, cardiovascular events, and drug interactions.
Which NSAIDs carry higher cardiovascular risk?
Diclofenac and COX-2 selective inhibitors are associated with increased risk of myocardial infarction and stroke.
Can NSAIDs delay fracture healing?
Yes, NSAIDs inhibit prostaglandins involved in bone formation, which may delay fracture healing and spinal fusion.
Why is ketorolac limited to short-term use?
Ketorolac has a high risk of gastrointestinal bleeding and kidney toxicity when used beyond short-term therapy.
Are NSAIDs safe in patients with heart disease?
NSAIDs should be used cautiously or avoided in heart disease due to increased risk of hypertension, heart failure, and thrombotic events.
Why should NSAIDs be avoided with anticoagulants like warfarin?
NSAIDs increase bleeding risk by inhibiting platelets and damaging gastric mucosa.
Can NSAIDs trigger asthma attacks?
Yes, in aspirin-sensitive individuals NSAIDs may trigger bronchospasm due to increased leukotriene production.
Are NSAIDs safe during pregnancy?
NSAIDs should be avoided in the third trimester due to risk of premature ductus arteriosus closure and fetal kidney injury.
What precautions should be taken when using NSAIDs long term?
Use the lowest effective dose, monitor kidney and liver function, assess cardiovascular risk, and consider gastroprotection with PPIs.
What is a safer alternative when NSAIDs are contraindicated?
Paracetamol, topical NSAIDs, physiotherapy, opioids (short-term), or disease-modifying drugs depending on the condition.
MCQ Test - NSAIDs Uses and Risks in Orthopedic Medicine and Pain Management Guide
Progress:
0/15
Time: 00:00
Test Results
0%
0/15
0
Correct Answers
0
Wrong Answers
00:00
Time Taken
0
Skipped