Medical Disclaimer: This is educational content only, not medical advice. Consult a licensed healthcare provider for diagnosis/treatment. Information based on sources like WHO/CDC guidelines (last reviewed: 2026-02-13).
This article is being expanded for more depth. Check back soon!
Percutaneous Coronary Intervention PCI Procedure Indications Steps Complications Management
Frequently Asked Questions
What is Percutaneous Coronary Intervention (PCI)?
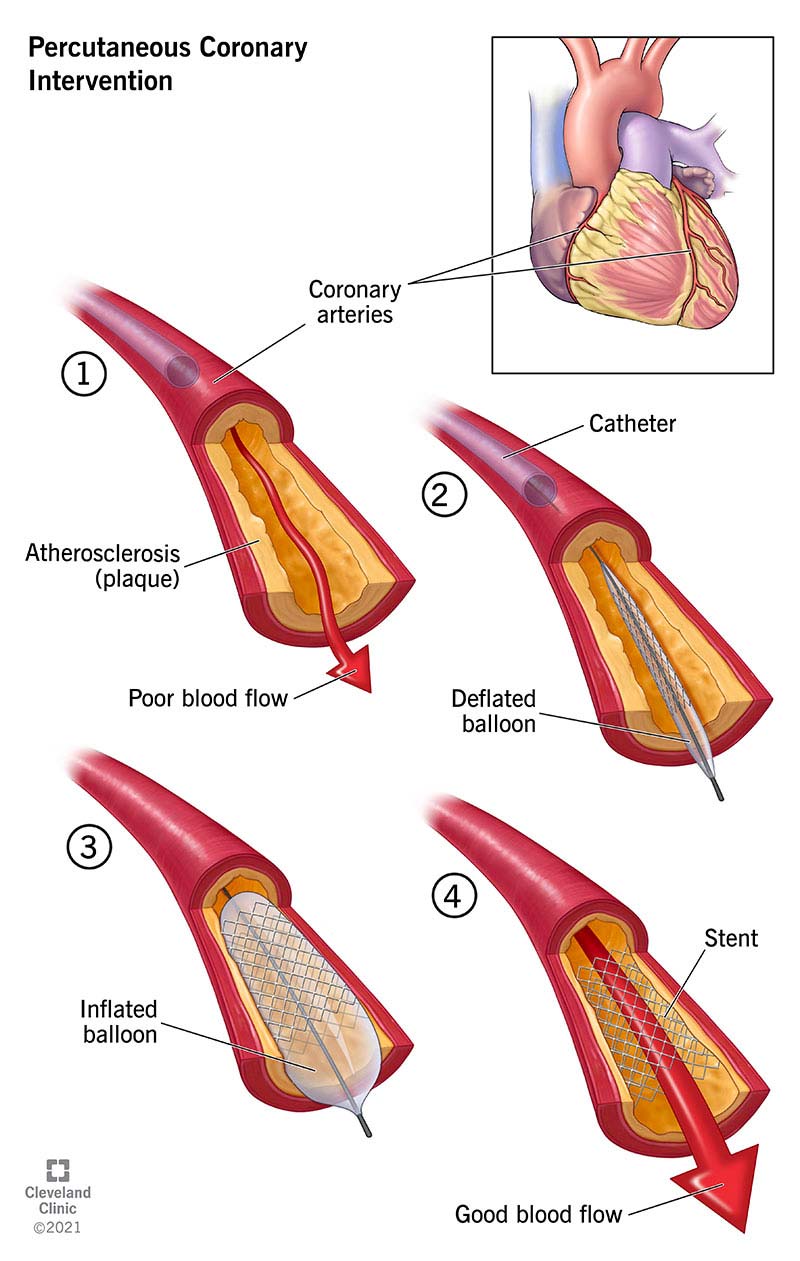
Percutaneous Coronary Intervention is a minimally invasive catheter-based procedure used to restore blood flow in narrowed or occluded coronary arteries, usually by balloon angioplasty followed by stent implantation.
What are the main indications for PCI?
PCI is indicated in ST-elevation myocardial infarction (primary PCI), high-risk NSTEMI or unstable angina, chronic stable angina with significant ischemia, and selected cases of left main or proximal LAD disease.
What is primary PCI?
Primary PCI refers to immediate PCI performed as the first reperfusion strategy in acute STEMI, ideally within 90–120 minutes of first medical contact.
What is the difference between PCI and coronary angioplasty?
Coronary angioplasty refers only to balloon dilatation of a coronary artery, whereas PCI includes angioplasty plus stent implantation and adjunctive pharmacotherapy.
What are drug-eluting stents (DES)?
Drug-eluting stents are coronary stents coated with antiproliferative drugs that inhibit neointimal hyperplasia, thereby reducing the risk of in-stent restenosis.
Why are drug-eluting stents preferred over bare-metal stents?
Drug-eluting stents significantly reduce restenosis rates compared to bare-metal stents, making them the standard of care in most PCI procedures.
What is dual antiplatelet therapy (DAPT)?
Dual antiplatelet therapy consists of aspirin plus a P2Y12 inhibitor (clopidogrel, prasugrel, or ticagrelor) to prevent stent thrombosis after PCI.
How long should DAPT be continued after PCI?
After PCI with drug-eluting stents, DAPT is recommended for at least 12 months in acute coronary syndrome and at least 6 months in stable coronary artery disease, unless bleeding risk is high.
What are the common access routes for PCI?
The common access routes for PCI are the radial artery and femoral artery, with radial access preferred due to lower bleeding complications.
What is the no-reflow phenomenon in PCI?
No-reflow is a complication where there is inadequate myocardial perfusion despite successful opening of the epicardial coronary artery, usually due to microvascular obstruction.
What are the major complications of PCI?
Major complications include stent thrombosis, coronary dissection or perforation, no-reflow phenomenon, contrast-induced nephropathy, bleeding, and vascular access complications.
What is contrast-induced nephropathy after PCI?
Contrast-induced nephropathy is acute kidney injury occurring after exposure to contrast media during PCI, characterized by a rise in serum creatinine within 48–72 hours.
When is CABG preferred over PCI?
CABG is preferred in patients with diabetes and multivessel disease, left main disease with high SYNTAX score, and complex coronary anatomy unsuitable for PCI.
What is in-stent restenosis?
In-stent restenosis is re-narrowing of a stented coronary segment due to neointimal hyperplasia, typically occurring months after PCI.
What is the most feared late complication of PCI?
Late stent thrombosis is the most feared late complication of PCI because it can lead to sudden myocardial infarction and death.
MCQ Test - Percutaneous Coronary Intervention PCI Procedure Indications Steps Complications Management
Progress:
0/15
Time: 00:00
Test Results
0%
0/15
0
Correct Answers
0
Wrong Answers
00:00
Time Taken
0
Skipped