Tricuspid Regurgitation (TR) — Complete Clinical Reference
Definition
Tricuspid regurgitation is the backward flow of blood from the right ventricle (RV) into the right atrium (RA) during systole due to incompetent tricuspid valve closure, leading to right-sided volume overload.
Anatomy & Normal Physiology (Brief)
- Tricuspid valve: 3 leaflets (anterior, posterior, septal)
- Located between RA and RV
- Prevents systolic backflow into RA
- Normal closure depends on leaflet integrity, chordae, papillary muscles, RV geometry, and annular size
Classification
1. Primary (Organic) TR
Structural abnormality of the valve apparatus itself.
2. Secondary (Functional) TR (most common)
Normal leaflets, but regurgitation due to RV dilation or tricuspid annular dilatation.
Etiology
Primary TR – Causes
- Rheumatic heart disease
- Infective endocarditis (IV drug use, pacemaker leads)
- Carcinoid syndrome
- Congenital (Ebstein anomaly)
- Trauma (chordal rupture)
- Iatrogenic (pacemaker/ICD leads)
- Myxomatous degeneration
- Radiation-induced valvular disease
Secondary TR – Causes
- Pulmonary hypertension (most common)
- Left-sided heart disease (mitral stenosis/regurgitation, LV failure)
- Right ventricular dilation (cardiomyopathy)
- Atrial fibrillation → RA dilation
- Chronic lung disease (cor pulmonale)
Pathophysiology
- Incompetent tricuspid valve → systolic backflow into RA
- RA volume overload → RA dilation
- Elevated RA pressure → systemic venous congestion
- Progressive RV dilation and dysfunction
- Reduced forward flow → low cardiac output symptoms in advanced disease
Clinical Features
Symptoms
- Often asymptomatic early
- Fatigue, weakness
- Abdominal fullness, bloating
- Right upper quadrant pain
- Peripheral edema
- Ascites
- Anorexia, nausea
Signs
General
- Raised jugular venous pressure (JVP) with prominent v wave
- Peripheral edema
- Ascites
- Hepatomegaly (pulsatile liver)
Cardiac Auscultation
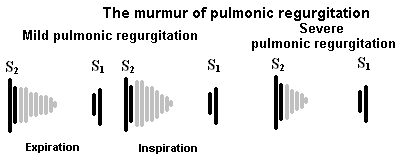
- Pansystolic murmur at left lower sternal border
- Murmur increases with inspiration (Carvallo sign)
- Often associated with:
* Loud P2 (pulmonary hypertension)
* RV S3
Investigations
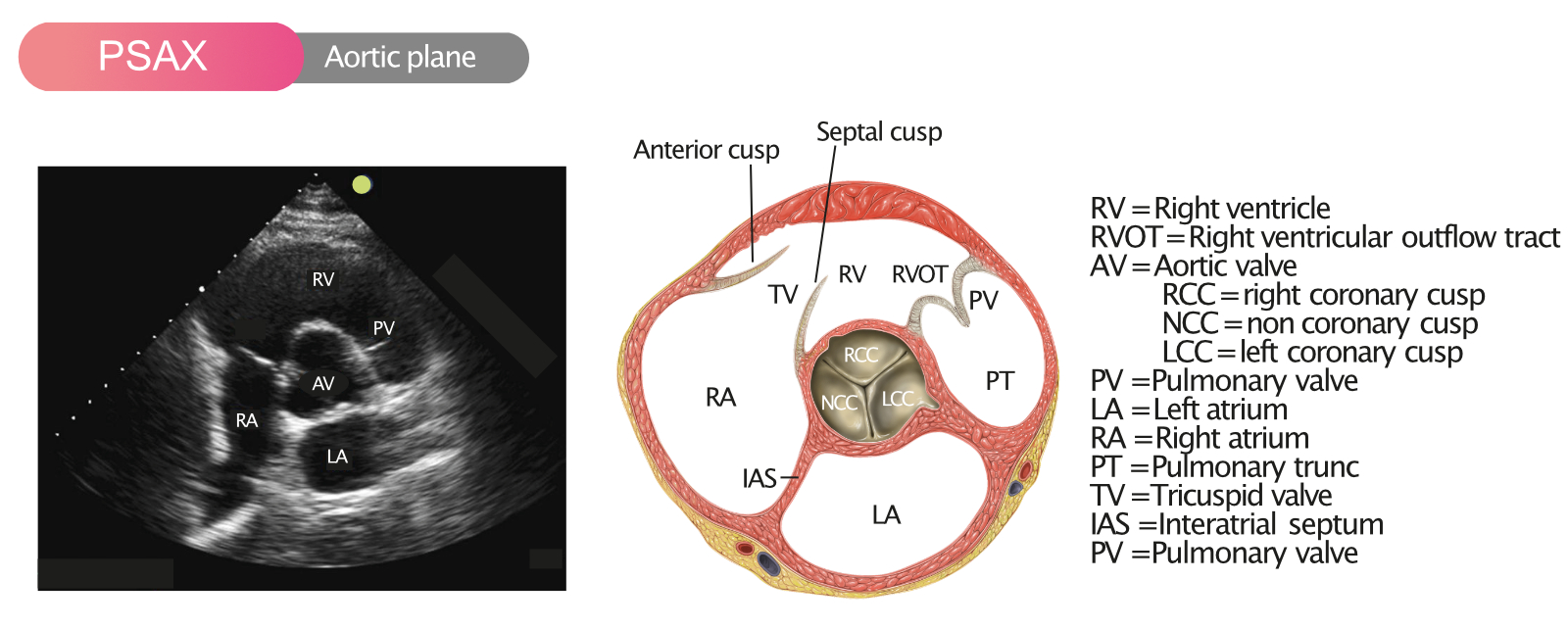
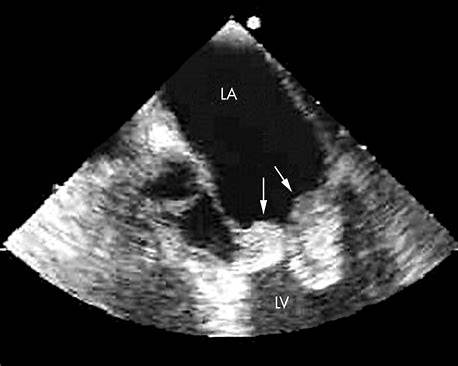
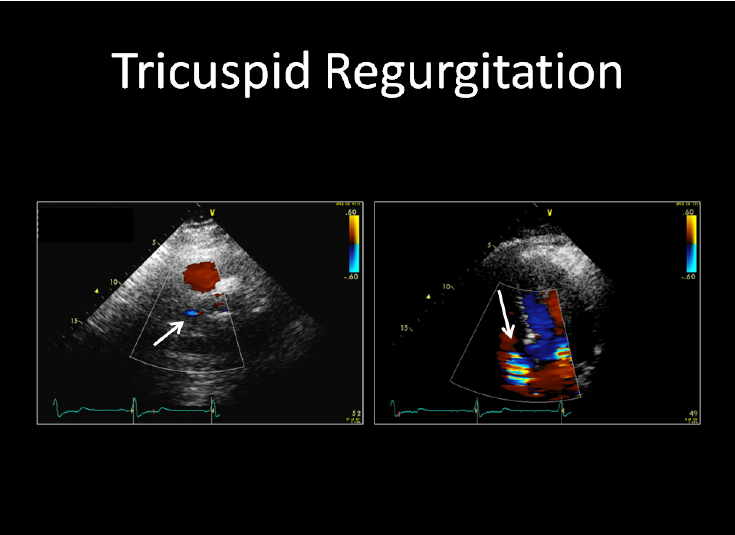
1. Echocardiography (Gold Standard)
- Color Doppler: regurgitant jet
- Annular dilatation (>40 mm)
- RV size and function
- RA enlargement
- Pulmonary artery pressure
- Etiology (leaflet abnormality vs functional)
2. ECG
- Right atrial enlargement
- Atrial fibrillation
- RV hypertrophy
3. Chest X-ray
- Cardiomegaly
- Enlarged RA
- Pulmonary artery enlargement
4. Cardiac MRI
- Accurate RV volume and function assessment (selected cases)
5. Cardiac Catheterization
- When diagnosis uncertain
- Pre-surgical evaluation
Severity Grading (Echo)
- Mild
- Moderate
- Severe
- Massive / Torrential (newer classification)
Differential Diagnosis
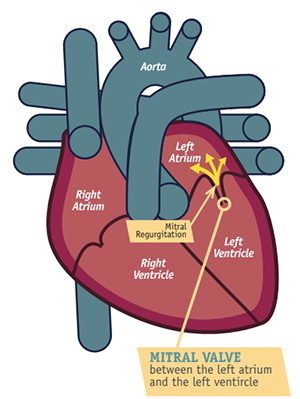
- Mitral regurgitation
- Constrictive pericarditis
- Restrictive cardiomyopathy
- Right heart failure of other causes
- Pulmonary hypertension without TR
Management
Principles
- Treat underlying cause
- Control volume overload
- Consider surgical/interventional repair when indicated
1. Medical Management
(Mainstay for most patients)
Diuretics
- Furosemide
* Indication: Volume overload
* Dose: 20–80 mg/day (oral/IV)
* Mechanism: Loop diuretic → Na⁺/water excretion
* Adverse effects: Hypokalemia, hypotension
* Monitoring: Electrolytes, renal function
* Counselling: Salt restriction, daily weight
Aldosterone antagonists
- Spironolactone
* Useful in ascites and edema
Treat precipitating causes
- Pulmonary hypertension therapy
- Rate/rhythm control in AF
- Treat left-sided valvular disease
2. Surgical / Interventional Management
Indications
- Severe TR with symptoms
- Progressive RV dilation/dysfunction
- TR during left-sided valve surgery
- Failure of medical therapy
Procedures
- Tricuspid valve repair (preferred)
* Annuloplasty ring
- Valve replacement
* Bioprosthetic preferred over mechanical
- Transcatheter tricuspid interventions
* Edge-to-edge repair (selected patients)
Special Clinical Associations
- Carcinoid syndrome → plaque-like fibrosis of valve
- Ebstein anomaly → congenital apical displacement
- IV drug users → infective endocarditis
- Pacemaker-related TR → lead impingement
Prognosis
- Mild TR: benign
- Severe untreated TR:
* Progressive right heart failure
* Reduced survival
- Prognosis depends on:
* RV function
* Pulmonary pressures
* Timing of intervention
Key Exam & Clinical Pearls
- TR murmur increases with inspiration
- Prominent v wave in JVP
- Functional TR is far more common than primary
- Always assess TR in left-sided valve disease
- Early repair improves outcomes
If you want next:
- SEO title, description, keywords
- High-level MCQs (case-based, hard)
- FAQ JSON
- Management algorithms
- Echo criteria tables
Just tell me.