Rheumatic Heart Disease (RHD)
1. Definition
Rheumatic Heart Disease is a chronic, progressive valvular heart disease resulting from immune-mediated damage following acute rheumatic fever (ARF), itself a sequela of untreated or inadequately treated Group A β-hemolytic streptococcal (GAS) pharyngitis. It predominantly affects the mitral valve, followed by the aortic valve, leading to stenosis, regurgitation, or mixed lesions.
2. Epidemiology
- Predominantly affects children and young adults in low- and middle-income countries
- Major cause of acquired heart disease in the young
- High burden in South Asia, Sub-Saharan Africa, Pacific Islands
- Female predominance (especially mitral stenosis)
3. Etiology and Risk Factors
Primary cause
- Autoimmune response to GAS pharyngitis
Risk factors
- Recurrent untreated sore throat
- Poverty, overcrowding
- Limited access to healthcare
- Poor adherence to secondary prophylaxis
- Genetic susceptibility (HLA associations)
4. Pathophysiology
- GAS infection → molecular mimicry
- Cross-reactive antibodies and T-cells target cardiac tissue
- Pancarditis during ARF
- Chronic inflammation → fibrosis, commissural fusion, leaflet thickening
- Progressive valvular deformity and dysfunction
Valve involvement (frequency)
- Mitral valve: ~70%
- Aortic valve: ~25%
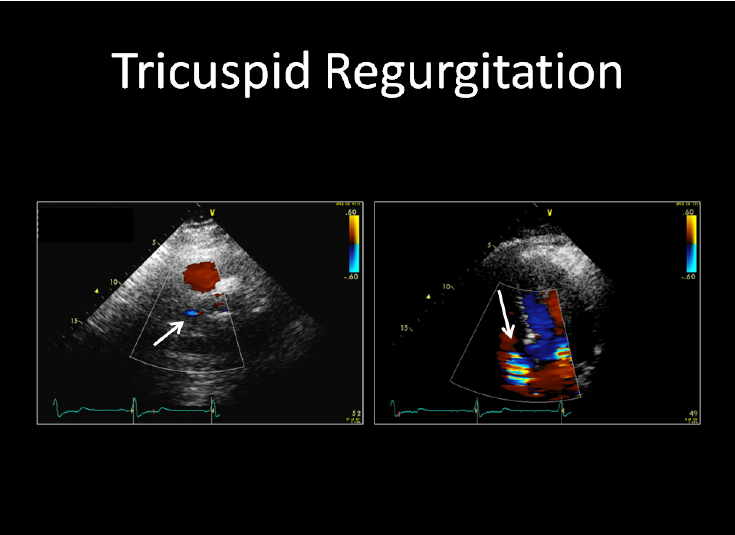
- Tricuspid valve: ~5% (usually secondary)
- Pulmonary valve: rare
5. Valve-Specific Lesions
Mitral stenosis
- Commissural fusion
- “Fish-mouth” valve
- Left atrial enlargement → atrial fibrillation → thromboembolism
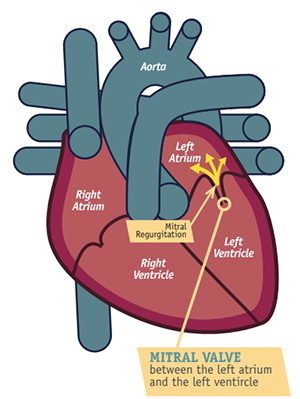
Mitral regurgitation
- Leaflet retraction
- Chordal elongation or rupture
Aortic stenosis
- Cusp thickening and fusion
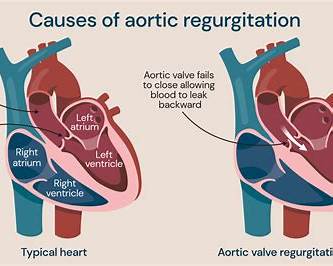
Aortic regurgitation
- Cusp retraction
6. Clinical Features
A. Acute Rheumatic Fever (preceding illness)
- Migratory polyarthritis
- Carditis (tachycardia, murmurs, cardiomegaly)
- Chorea
- Subcutaneous nodules
- Erythema marginatum
B. Chronic Rheumatic Heart Disease
Depends on valve involved:
Mitral stenosis
- Dyspnea, orthopnea, PND
- Hemoptysis
- Palpitations (AF)
- Stroke or systemic embolism
Mitral regurgitation
- Fatigue
- Dyspnea
- Signs of left ventricular failure
Aortic valve disease
- Exertional dyspnea
- Angina
- Syncope (AS)
- Bounding pulse (AR)
Advanced disease
- Right heart failure
- Ascites, pedal edema
- Cachexia
7. Physical Examination
General
- Malar flush (mitral stenosis)
- Irregularly irregular pulse (AF)
Cardiac auscultation
- MS: Loud S1, opening snap, mid-diastolic murmur
- MR: Pansystolic murmur at apex radiating to axilla
- AS: Ejection systolic murmur radiating to carotids
- AR: Early diastolic decrescendo murmur
8. Investigations
A. Laboratory
- Evidence of prior streptococcal infection:
* Elevated ASO titre
* Anti-DNase B
- Inflammatory markers (during ARF)
B. ECG
- Atrial fibrillation
- Left atrial enlargement
- Ventricular hypertrophy
C. Chest X-ray
- Cardiomegaly
- Left atrial enlargement
- Pulmonary congestion
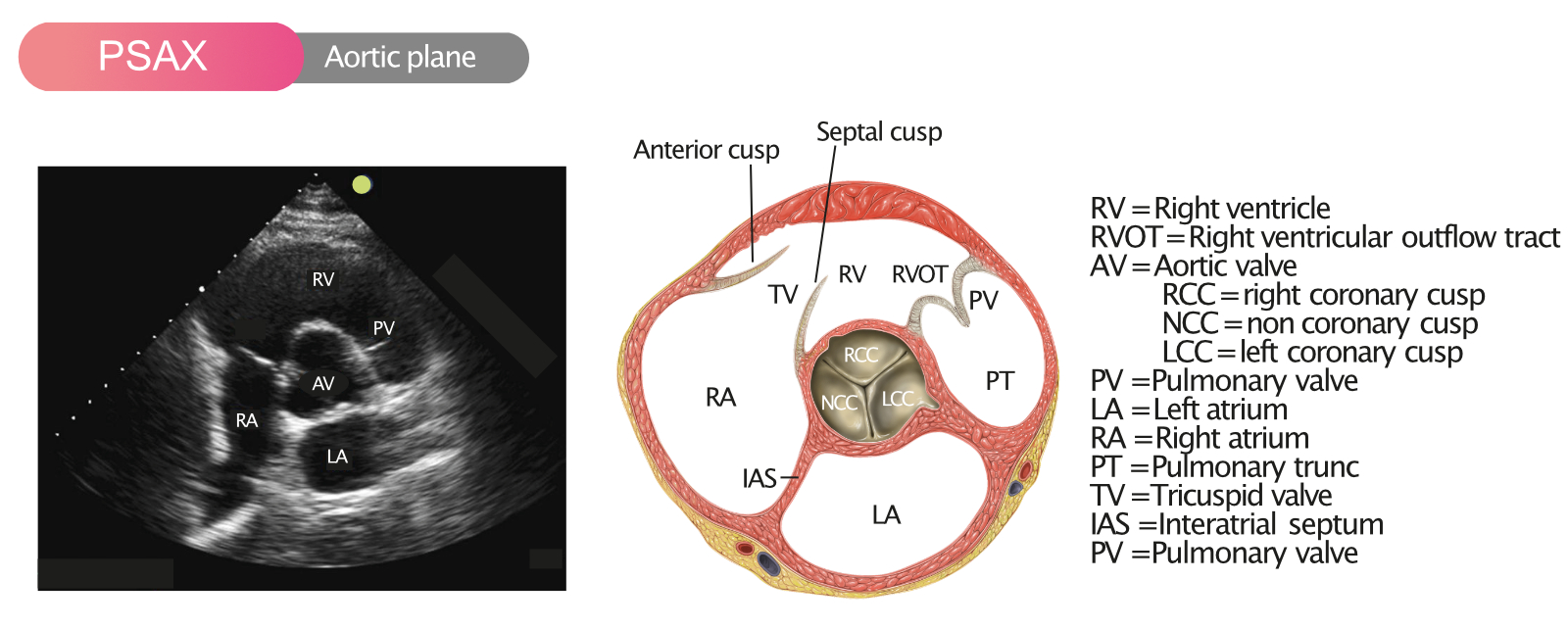
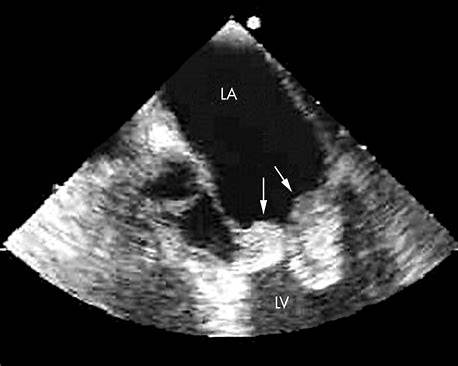
D. Echocardiography (gold standard)
- Valve morphology
- Severity of stenosis/regurgitation
- Chamber sizes
- Pulmonary artery pressure
- Detection of LA thrombus
E. Transesophageal Echo
- Before cardioversion or balloon valvotomy
9. Diagnostic Criteria
Jones Criteria for Acute Rheumatic Fever:
- Major: Carditis, polyarthritis, chorea, erythema marginatum, subcutaneous nodules
- Minor: Fever, arthralgia, elevated ESR/CRP, prolonged PR interval
- Plus evidence of recent GAS infection
10. Differential Diagnosis
- Degenerative valvular disease
- Congenital valve disease
- Infective endocarditis
- Dilated cardiomyopathy
- Hypertrophic cardiomyopathy
11. Management
A. Acute Rheumatic Fever
1. Eradication of GAS
Benzathine penicillin G
- Indication: Confirmed or suspected GAS infection
- Dose:
* Adults: 1.2 million units IM single dose
* Children <27 kg: 600,000 units IM
- MOA: Inhibits bacterial cell wall synthesis
- Adverse effects: Allergy, anaphylaxis
- Contraindications: Penicillin allergy
- Alternative: Azithromycin or erythromycin
2. Anti-inflammatory therapy
Aspirin
- Dose: 60–100 mg/kg/day in divided doses
- Indication: Arthritis
- Adverse effects: Gastritis, bleeding
- Monitoring: Salicylate toxicity
Corticosteroids
- Indication: Severe carditis with heart failure
- Example: Prednisolone 1–2 mg/kg/day
B. Chronic Rheumatic Heart Disease
1. Secondary Prophylaxis (most critical)
Benzathine penicillin G
- Dose: 1.2 million units IM every 3–4 weeks
- Duration:
* No carditis: 5 years or until age 21
* Carditis, no residual disease: 10 years or until 21
* Residual valvular disease: ≥10 years or lifelong
2. Medical Management (symptom-based)
Diuretics (e.g., Furosemide)
- Indication: Congestive symptoms
- MOA: Loop diuretic
- Monitoring: Electrolytes
Beta-blockers
- Indication: Rate control in AF, MS
- Example: Metoprolol
Digoxin
- Indication: AF with heart failure
- Monitoring: Serum levels, toxicity
Anticoagulation
- Indication:
* AF
* Prior embolism
* LA thrombus
- Drug: Warfarin
- Target INR: 2.0–3.0
- Contraindications: Pregnancy (1st trimester)
3. Interventional and Surgical Management
Percutaneous balloon mitral valvotomy
- Indication: Symptomatic severe MS with favorable valve anatomy
- Contraindications: LA thrombus, significant MR
Valve repair or replacement
- Indications:
* Severe symptomatic valve disease
* LV dysfunction
- Mechanical valve → lifelong anticoagulation
- Bioprosthetic valve → limited durability
12. Complications
- Atrial fibrillation
- Thromboembolism
- Infective endocarditis
- Heart failure
- Pulmonary hypertension
- Stroke
13. Prognosis
- Depends on:
* Severity of valve involvement
* Adherence to secondary prophylaxis
* Timely intervention
- Early detection and prophylaxis dramatically reduce progression
14. Prevention
Primary prevention
- Early diagnosis and treatment of streptococcal pharyngitis
Secondary prevention
- Long-term penicillin prophylaxis
Public health measures
- Improved living conditions
- Access to primary healthcare
- School-based sore throat programs
15. Key Clinical Pearls
- Mitral stenosis in a young patient → think RHD
- Secondary prophylaxis saves valves and lives
- Echocardiography is essential even in asymptomatic patients
- AF + RHD = anticoagulate unless contraindicated