Infective Endocarditis – Complete Clinical Reference
Definition
Infective endocarditis (IE) is a microbial infection of the endocardial surface of the heart, most commonly involving cardiac valves (native or prosthetic), but may also affect mural endocardium, chordae tendineae, or intracardiac devices.
Pathophysiology
- Endothelial injury (turbulent flow, prosthetic material)
- Platelet–fibrin deposition → non-bacterial thrombotic endocarditis
- Transient bacteremia/fungemia
- Microbial adherence to thrombus
- Vegetation formation
- Local destruction + systemic embolization + immune complex phenomena
Etiology and Causative Organisms
Common Organisms
| Setting | Organisms |
| ------------------------------ | ------------------------------------------------ |
| Native valve (community) | Viridans streptococci, Staphylococcus aureus |
| Healthcare-associated | S. aureus, Enterococci |
| Prosthetic valve (early <1 yr) | S. epidermidis, S. aureus, Gram-negatives |
| Prosthetic valve (late >1 yr) | Similar to native valve |
| IV drug users | S. aureus (often tricuspid) |
| Culture-negative | Coxiella burnetii, Bartonella, HACEK |
HACEK Group
- Haemophilus
- Aggregatibacter
- Cardiobacterium
- Eikenella
- Kingella
Risk Factors
- Rheumatic or degenerative valve disease
- Prosthetic valves
- Congenital heart disease
- Previous infective endocarditis
- IV drug use
- Indwelling catheters
- Immunosuppression
Classification
By Valve
- Native valve endocarditis (NVE)
- Prosthetic valve endocarditis (PVE)
By Course
- Acute (rapid, destructive – S. aureus)
- Subacute (indolent – viridans streptococci)
Clinical Features
Constitutional
- Fever (most common)
- Chills, malaise
- Weight loss, night sweats
Cardiac
- New or changing murmur
- Acute heart failure
- Conduction block (suggests abscess)
Vascular Phenomena
- Janeway lesions (painless palms/soles)
- Splinter hemorrhages
- Arterial emboli
- Pulmonary emboli (right-sided IE)
Immunologic Phenomena
- Osler nodes (painful fingers/toes)
- Roth spots
- Glomerulonephritis
- Positive rheumatoid factor
Other
- Stroke
- Hematuria
- Splenomegaly
Investigations
Blood Cultures (Cornerstone)
- 3 sets from different sites
- Before antibiotics
- Positive in >90%
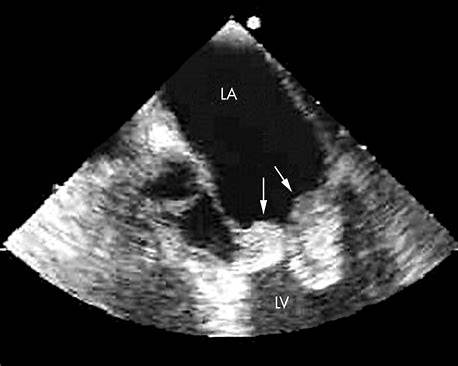
Echocardiography
- TTE – initial
- TEE – gold standard
(prosthetic valves, abscess, poor TTE window)
Laboratory
- Normocytic normochromic anemia
- Raised ESR, CRP
- Microscopic hematuria
- Low complement levels
Imaging (Complications)
- CT/MRI brain – embolic stroke
- CT chest – septic emboli
- PET-CT – prosthetic valve infection
Diagnosis – Modified Duke Criteria
Major Criteria
- Positive blood cultures with typical organism
- Evidence of endocardial involvement (echo or new regurgitation)
Minor Criteria
- Predisposition
- Fever ≥38°C
- Vascular phenomena
- Immunologic phenomena
- Microbiological evidence not meeting major
Definite IE
- 2 major
OR
- 1 major + 3 minor
OR
- 5 minor
Differential Diagnosis
- Acute rheumatic fever
- Libman–Sacks endocarditis
- Marantic (non-bacterial) endocarditis
- Vasculitis
- Malignancy-associated fever
- Atrial myxoma
Management (Stepwise)
1. General Measures
- Hospital admission
- Strict bed rest (initial phase)
- Treat heart failure, arrhythmias
- Remove infected devices
2. Empiric Antibiotic Therapy
(Start after blood cultures)
Native Valve (Community-acquired)
- Ceftriaxone + Vancomycin
Prosthetic Valve / Healthcare-associated
- Vancomycin + Gentamicin + Rifampicin
Targeted Antimicrobial Therapy (Key Drugs)
Vancomycin
- Indication: MRSA, penicillin-allergic
- MOA: Inhibits cell wall synthesis
- Dose: 15–20 mg/kg IV every 8–12 h
- Adverse effects: Nephrotoxicity, red man syndrome
- Monitoring: Trough levels, renal function
- Contraindication: Severe hypersensitivity
- Counseling: Slow infusion, hydration
Ceftriaxone
- Indication: Streptococci, HACEK
- MOA: β-lactam cell wall inhibition
- Dose: 2 g IV once daily
- Adverse effects: Biliary sludge, allergy
- Contraindication: Severe cephalosporin allergy
Gentamicin
- Indication: Synergy (Enterococcus)
- MOA: 30S ribosomal inhibition
- Dose: 1 mg/kg IV every 8 h
- Adverse effects: Nephrotoxicity, ototoxicity
- Monitoring: Drug levels, renal function
- Contraindication: Renal failure (relative)
Rifampicin
- Indication: Prosthetic valve IE
- MOA: RNA polymerase inhibition
- Dose: 300–600 mg orally/IV every 12 h
- Adverse effects: Hepatotoxicity, orange discoloration
- Interactions: Induces CYP450 (↓ warfarin, OCPs)
- Monitoring: LFTs
Duration of Therapy
- Native valve: 4–6 weeks
- Prosthetic valve: ≥6 weeks
Indications for Surgery
Absolute
- Acute heart failure due to valve dysfunction
- Uncontrolled infection (abscess, persistent bacteremia)
- Large vegetations with recurrent emboli
- Prosthetic valve dehiscence
Relative
- Vegetation >10 mm
- Fungal endocarditis
- Resistant organisms
Complications
- Heart failure (most common cause of death)
- Stroke
- Septic emboli
- Mycotic aneurysm
- Valvular destruction
- Renal failure
- Conduction abnormalities
Prognosis
- Mortality: 15–30%
- Worse with:
S. aureus*
* Prosthetic valve
* Heart failure
* Delayed treatment
Prevention (Antibiotic Prophylaxis – High Risk Only)
High-Risk Patients
- Prosthetic valves
- Previous IE
- Certain congenital heart diseases
Dental Procedures
- Amoxicillin 2 g orally 30–60 min before
- Clindamycin 600 mg if penicillin-allergic
1. IV Drug User with Fever and Hemoptysis
Scenario: 28-year-old IV drug user, fever, pleuritic chest pain, hemoptysis. Echo: tricuspid vegetations.
Diagnosis: Right-sided IE (likely Staphylococcus aureus)
Management:
- IV vancomycin (or anti-staphylococcal beta-lactam if MSSA)
- Treat septic pulmonary emboli
- Surgery only if persistent bacteremia, large vegetations, or RV failure
2. Native Valve IE after Dental Extraction
Scenario: Fever 3 weeks after dental work, new murmur.
Organism: Viridans streptococci
Management:
- IV ceftriaxone or penicillin G for 4 weeks
- No surgery unless complications
3. Prosthetic Valve with Persistent Fever
Scenario: Mechanical valve, fever despite antibiotics, TEE shows abscess.
Diagnosis: Prosthetic valve endocarditis
Management:
- Vancomycin + gentamicin + rifampicin
- Urgent surgery (abscess = absolute indication)
4. Culture-Negative IE after Antibiotics
Scenario: Fever, negative cultures, prior antibiotic exposure.
Management:
- Stop antibiotics if safe → repeat cultures
- Empiric therapy covering fastidious organisms
- Serology for Coxiella, Bartonella
5. IE with Acute Heart Failure
Scenario: Acute pulmonary edema, severe MR on echo.
Cause: Valve destruction/chordal rupture
Management:
- Stabilize heart failure
- Emergency valve surgery
6. IE with Stroke
Scenario: IE patient develops sudden hemiparesis.
Management:
- CT brain (exclude hemorrhage)
- Continue antibiotics
- Surgery delayed 2–4 weeks unless heart failure or uncontrolled infection
7. Enterococcal Endocarditis
Scenario: Elderly patient, urinary source, positive Enterococcus cultures.
Management:
- Ampicillin + gentamicin OR ampicillin + ceftriaxone
- Duration: 6 weeks
8. Fungal Endocarditis
Scenario: Immunocompromised patient, large vegetations, Candida species.
Management:
- IV amphotericin B or echinocandin
- Early surgery mandatory
9. IE with New Conduction Block
Scenario: PR prolongation / heart block in IE.
Cause: Perivalvular abscess
Management:
- TEE urgently
- Early surgery
10. Recurrent Emboli despite Antibiotics
Scenario: Vegetation >10 mm, repeated emboli.
Management:
- Early surgical intervention
11. Right-Sided IE with Good Response
Scenario: Tricuspid IE, fever resolving.
Management:
- Continue IV antibiotics
- Surgery usually not required
12. IE with Renal Failure and Hematuria
Scenario: Hematuria, RBC casts.
Diagnosis: Immune complex GN
Management:
- Treat IE with antibiotics
- Avoid nephrotoxic drugs
- Dialysis if needed
13. Early Prosthetic Valve IE (<1 year)
Scenario: Fever 3 months post valve surgery.
Organism: Staphylococcus epidermidis
Management:
- Vancomycin + gentamicin + rifampicin
- Usually requires surgery
14. Late Prosthetic Valve IE (>1 year)
Scenario: Fever 2 years post surgery.
Management:
- Treat similar to native valve IE
- Surgery based on complications
15. HACEK Endocarditis
Scenario: Subacute IE, slow-growing Gram-negative bacilli.
Management:
- IV ceftriaxone for 4 weeks
16. IE in Congenital Heart Disease
Scenario: Unrepaired VSD, fever, murmur.
Management:
- Prolonged IV antibiotics
- Surgery if hemodynamic compromise
17. IE with Splenic Abscess
Scenario: Left upper quadrant pain, fever.
Management:
- IV antibiotics
- Percutaneous drainage or splenectomy if rupture risk
18. IE with Mycotic Aneurysm
Scenario: Severe headache, focal deficit.
Management:
- Neuroimaging
- Antibiotics
- Neurosurgical intervention if rupture risk
19. IE in Pregnancy
Scenario: Pregnant woman with IE.
Management:
- Safe IV antibiotics (avoid aminoglycosides if possible)
- Surgery only if life-threatening
20. IE with Persistent Bacteremia
Scenario: Positive cultures after 7 days therapy.
Management:
- Review antibiotic sensitivity
- Search for abscess
- Surgery often required
21. IE with Large Mobile Vegetation on Mitral Valve
Scenario: >15 mm vegetation.
Management:
- Early surgery even without emboli
22. IE in Hemodialysis Patient
Scenario: AV fistula, S. aureus bacteremia.
Management:
- IV vancomycin
- Remove infected access
- High threshold for surgery
23. Recurrent IE
Scenario: History of previous IE.
Management:
- Full IV antibiotics
- Strong consideration for valve replacement
24. IE with Severe Anemia and Splenomegaly
Scenario: Chronic IE.
Management:
- Treat infection
- Supportive care (transfusion if needed)
25. Suspected IE with Normal Initial Echo
Scenario: High clinical suspicion, negative TTE.
Management:
- Perform TEE
- Repeat echo if needed
- Continue diagnostic work-up