Mitral Regurgitation (MR): Complete Clinical Guide and Detailed Management
1. Definition
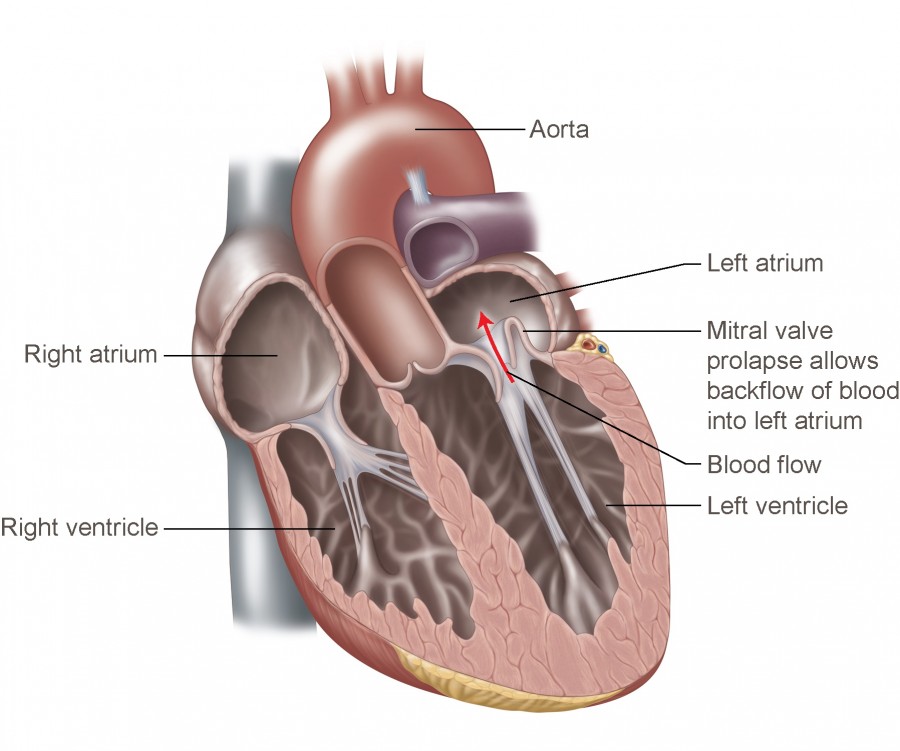
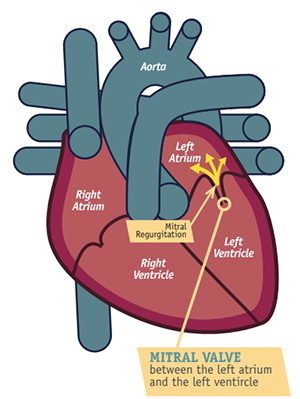
Mitral regurgitation is a valvular heart disease in which incomplete closure of the mitral valve during systole causes retrograde flow of blood from the left ventricle (LV) into the left atrium (LA).
2. Classification
A. By Etiology
1. Primary (Organic) MR
- Structural abnormality of valve apparatus
- Causes:
* Myxomatous degeneration (MVP – most common)
* Rheumatic heart disease
* Infective endocarditis
* Chordae tendineae rupture
* Papillary muscle rupture
* Congenital cleft mitral valve
2. Secondary (Functional) MR
- Valve structurally normal
- Due to LV remodeling
- Causes:
* Ischemic cardiomyopathy
* Dilated cardiomyopathy
* LV aneurysm
B. By Time Course
- Acute MR
- Chronic MR → compensated → decompensated
3. Pathophysiology
Acute MR
- Sudden regurgitation → small, non-compliant LA
- Rapid ↑ LA pressure → pulmonary edema
- No time for LV or LA adaptation
- ↓ Forward cardiac output → shock
Chronic MR
- Gradual volume overload
- LA dilation → ↓ pulmonary congestion initially
- LV eccentric hypertrophy
- Eventually → LV systolic dysfunction
4. Causes (Etiology)
Acute MR Causes
- Papillary muscle rupture (post-MI)
- Chordal rupture
- Acute infective endocarditis
- Blunt chest trauma
Chronic MR Causes
- Mitral valve prolapse
- Rheumatic disease
- Dilated cardiomyopathy
- Ischemic heart disease
- Annular calcification
5. Clinical Features
Symptoms
- Dyspnea on exertion
- Orthopnea, PND
- Fatigue
- Palpitations (AF)
- Hemoptysis (late)
- Acute MR: sudden severe breathlessness
Signs
- Apex displaced down and out
- Hyperdynamic apex beat
- Holosystolic murmur at apex → radiates to axilla
- Soft S1
- S3 gallop (volume overload)
- AF signs in chronic MR
6. Investigations
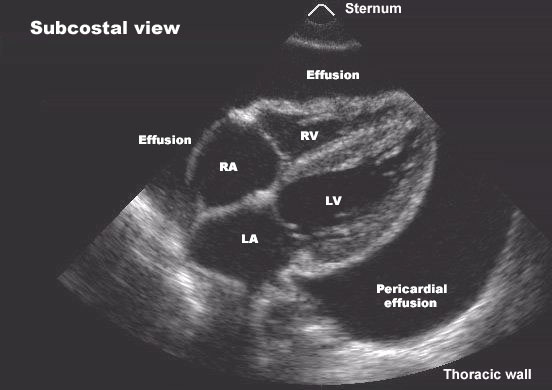
A. Echocardiography (Gold Standard)
- Valve anatomy
- MR severity
- LV size and EF
- Pulmonary artery pressure
Severity parameters
- Regurgitant volume ≥60 mL
- EROA ≥0.40 cm²
- Vena contracta ≥0.7 cm
B. ECG
- LA enlargement
- Atrial fibrillation
- LV hypertrophy
C. Chest X-ray
- LA and LV enlargement
- Pulmonary congestion
D. Cardiac MRI
- Precise MR quantification when echo unclear
E. Cardiac Catheterization
- Pre-surgical coronary assessment
7. Differential Diagnosis
- Tricuspid regurgitation
- Ventricular septal defect
- Hypertrophic cardiomyopathy
- Aortic regurgitation (flow murmur)
8. MANAGEMENT OF MITRAL REGURGITATION (CORE SECTION)
Management depends on:
- Acute vs chronic
- Severity
- Symptoms
- LV function
- Etiology
A. Acute Severe Mitral Regurgitation (Medical Emergency)
Immediate Management
- Oxygen / Non-invasive ventilation
- Reduce afterload
- Reduce pulmonary congestion
- Urgent surgery
Drugs Used (With Full Details)
1. Nitroprusside
- Indication: Acute severe MR with pulmonary edema
- MOA: Arterial and venous vasodilation → ↓ afterload → ↓ regurgitation
- Dose: 0.25–5 µg/kg/min IV infusion
- Adverse effects: Hypotension, cyanide toxicity
- Monitoring: BP, acid–base status
- Contraindication: Hypotension
2. Loop Diuretics (Furosemide)
- MOA: ↓ preload → ↓ pulmonary congestion
- Dose: 20–80 mg IV
- Adverse effects: Hypokalemia, dehydration
- Monitoring: Electrolytes, urine output
3. Inotropes (If shock)
- Dobutamine
* Dose: 2–20 µg/kg/min
* Improves forward flow
Definitive Treatment
➡ Emergency mitral valve surgery (repair preferred)
B. Chronic Mitral Regurgitation
1. Asymptomatic Mild–Moderate MR
- No surgery
- Annual echocardiography
- Endocarditis prevention education
2. Chronic Severe MR (Medical Therapy)
> Medical therapy does NOT cure MR
> It stabilizes patients until surgery
Key Drug Classes
1. ACE Inhibitors (Enalapril / Ramipril)
- Indication: LV dysfunction, functional MR
- MOA: ↓ afterload → ↓ regurgitant volume
- Dose:
* Enalapril: 2.5–20 mg/day
- Adverse effects: Cough, hyperkalemia
- Contraindication: Pregnancy, bilateral RAS
- Monitoring: BP, creatinine, K⁺
2. Beta-Blockers (Metoprolol, Carvedilol)
- Indication: Functional MR, AF rate control
- MOA: ↓ myocardial oxygen demand, reverse remodeling
- Dose:
* Metoprolol: 25–200 mg/day
- Adverse effects: Bradycardia, fatigue
- Contraindication: Acute decompensated HF
3. Diuretics
- Symptomatic relief of congestion
4. Anticoagulation
Indication
- MR with atrial fibrillation
- LA thrombus
Warfarin
- INR target: 2–3
C. Surgical Management (Definitive Treatment)
Indications for Surgery (Class I)
- Symptomatic severe MR
- Asymptomatic severe MR with:
* LVEF ≤60%
* LVESD ≥40 mm
* New-onset AF
* Pulmonary hypertension
Surgical Options
1. Mitral Valve Repair (Preferred)
- Lower mortality
- Preserves LV function
- No long-term anticoagulation
2. Mitral Valve Replacement
- When repair not feasible
- Mechanical vs bioprosthetic valve
D. Transcatheter Therapy
MitraClip (Edge-to-Edge Repair)
- For high surgical risk patients
- Severe symptomatic functional MR
- Improves quality of life
9. Special Situations
MR + Atrial Fibrillation
- Rate control (beta blockers)
- Anticoagulation mandatory
MR in Pregnancy
- Usually tolerated if LV function normal
- Avoid ACE inhibitors
10. Prognosis
- Excellent with timely repair
- Poor if LV dysfunction develops before surgery
- Functional MR has worse outcomes
11. Patient Counselling Points
- Importance of follow-up echo
- Symptom recognition
- AF and stroke risk awareness
- Post-valve surgery anticoagulation compliance
12. Authoritative External References (For Deep Reading)
- ACC/AHA Valve Guidelines
https://www.acc.org/guidelines
- ESC Valvular Heart Disease Guidelines
https://www.escardio.org/Guidelines
- UpToDate – Mitral Regurgitation
https://www.uptodate.com/contents/mitral-regurgitation
- European Heart Journal Review
https://academic.oup.com/eurheartj
- StatPearls MR Review
https://www.ncbi.nlm.nih.gov/books/NBK532908/
If you want next:
- 25 high-level case scenarios with management
- Hard case-based MCQs (JSON or HTML exam UI)
- Comparison table: Acute vs Chronic MR
- Surgical decision algorithms
Just tell me 👍
Below are 20 detailed, exam-oriented and clinically realistic case scenarios on Mitral Regurgitation, each with diagnosis reasoning and appropriate management, suitable for UG/PG exams, ward teaching, and viva.
1. Acute MR After Myocardial Infarction
Scenario:
A 65-year-old man develops sudden severe dyspnea and hypotension 3 days after inferior wall MI. Chest auscultation reveals a new loud pansystolic murmur. Echo shows flail posterior mitral leaflet and normal-sized LA.
Diagnosis: Acute severe MR due to papillary muscle rupture.
Management: Oxygen, IV diuretics, IV nitroprusside if BP permits, inotropes if shock → emergency mitral valve surgery.
2. Chronic MR With Preserved LV Function
Scenario:
A 45-year-old woman with known mitral valve prolapse presents for routine follow-up. She is asymptomatic. Echo shows severe MR, LVEF 65%, LVESD 36 mm.
Diagnosis: Asymptomatic severe chronic MR with preserved LV function.
Management: Close follow-up with 6–12 monthly echocardiography; no surgery yet.
3. Asymptomatic MR With LV Dilatation
Scenario:
A 52-year-old man with severe MR is asymptomatic. Echo shows LVEF 58% and LVESD 42 mm.
Diagnosis: Severe MR with early LV systolic dysfunction.
Management: Mitral valve surgery indicated despite absence of symptoms.
4. MR With Atrial Fibrillation
Scenario:
A 60-year-old woman with chronic MR presents with palpitations. ECG shows atrial fibrillation. LA is markedly enlarged.
Diagnosis: Chronic MR complicated by AF.
Management: Rate control (beta blocker), oral anticoagulation, evaluate for valve surgery.
5. Functional MR in Dilated Cardiomyopathy
Scenario:
A 68-year-old man with heart failure has moderate-to-severe MR. Echo shows dilated LV, normal valve leaflets, tethering of mitral apparatus.
Diagnosis: Secondary (functional) MR.
Management: Optimal heart failure therapy (ACEI, beta blocker, MRA); consider MitraClip if symptoms persist.
6. Acute MR Due to Infective Endocarditis
Scenario:
A 40-year-old IV drug user presents with fever, pulmonary edema, and a new systolic murmur. Echo shows vegetation with leaflet perforation.
Diagnosis: Acute MR due to infective endocarditis.
Management: IV antibiotics + urgent surgery if heart failure persists.
7. MR With Pulmonary Hypertension
Scenario:
A patient with severe MR is asymptomatic but echo shows PASP 55 mmHg.
Diagnosis: Severe MR with pulmonary hypertension.
Management: Mitral valve surgery indicated (Class I indication).
8. Pregnancy With MR
Scenario:
A 28-year-old pregnant woman with known chronic MR presents at 24 weeks gestation. She is asymptomatic, LV function normal.
Diagnosis: Well-compensated MR in pregnancy.
Management: Observation; diuretics if congestion; avoid ACE inhibitors.
9. MR With Hemoptysis and Hoarseness
Scenario:
A patient with long-standing MR develops hemoptysis and hoarseness of voice.
Diagnosis: Severe MR with left atrial enlargement causing Ortner syndrome.
Management: Surgical correction of MR.
10. Acute MR With Cardiogenic Shock
Scenario:
A patient presents with flash pulmonary edema, hypotension, cold extremities, and soft systolic murmur.
Diagnosis: Acute severe MR with cardiogenic shock.
Management: Ventilatory support, afterload reduction, inotropes → emergency surgery.
11. MR With Preserved EF but Low Output
Scenario:
A patient with severe MR has LVEF 65% but complains of fatigue and low exercise tolerance.
Diagnosis: Preserved EF masking reduced forward cardiac output.
Management: Early surgical referral before EF declines.
12. MR After Chordal Rupture
Scenario:
A patient with long-standing MVP suddenly develops dyspnea. Echo shows ruptured chordae.
Diagnosis: Acute on chronic MR due to chordal rupture.
Management: Stabilization followed by mitral valve repair.
13. MR With Recurrent Pulmonary Edema
Scenario:
A 58-year-old man has recurrent hospitalizations for pulmonary edema. Echo shows severe MR and LVEF 55%.
Diagnosis: Symptomatic severe MR.
Management: Mitral valve surgery regardless of EF.
14. MR With Normal Murmur Intensity
Scenario:
A patient with acute MR has severe pulmonary edema but only a soft systolic murmur.
Diagnosis: Acute MR with rapid LA pressure equalization.
Management: Treat as medical emergency; echo-based diagnosis critical.
15. MR With LV Dysfunction
Scenario:
A patient with chronic MR has LVEF 45%.
Diagnosis: Decompensated chronic MR.
Management: Surgery still beneficial but prognosis worse due to delayed referral.
16. MR and Stroke
Scenario:
A patient with MR and atrial fibrillation presents with ischemic stroke.
Diagnosis: Cardioembolic stroke due to AF in MR.
Management: Anticoagulation + evaluation for valve intervention.
17. Ischemic MR After MI
Scenario:
A patient post-MI has moderate MR due to papillary muscle displacement.
Diagnosis: Ischemic functional MR.
Management: Optimal medical therapy ± revascularization; consider MitraClip if severe.
18. MR With S3 Gallop
Scenario:
A patient with MR has S3 on auscultation and displaced apex beat.
Diagnosis: Volume overload with LV dilation.
Management: Diuretics for symptoms; surgical evaluation.
19. Delayed Surgery Consequence
Scenario:
A patient refuses surgery for years and later presents with EF 35%.
Diagnosis: Advanced MR with irreversible LV dysfunction.
Management: Surgery possible but recovery limited; poor prognosis.
20. High Surgical Risk MR Patient
Scenario:
An elderly patient with severe MR and multiple comorbidities remains symptomatic despite medical therapy.
Diagnosis: Severe MR with high surgical risk.
Management: Transcatheter edge-to-edge repair (MitraClip).