Quick rules that help instantly (right-sided murmurs)
- Right-sided murmurs generally get louder with inspiration (↑ venous return to right heart) — classic for TR and often TS/PS too. ([MSD Manuals][1])
- Handgrip ↑ afterload → tends to increase regurgitant murmurs (more for left-sided; TR may rise variably).
- Valsalva release / squatting (↑ preload) can increase ejection murmurs (e.g., PS). ([MSD Manuals][2])
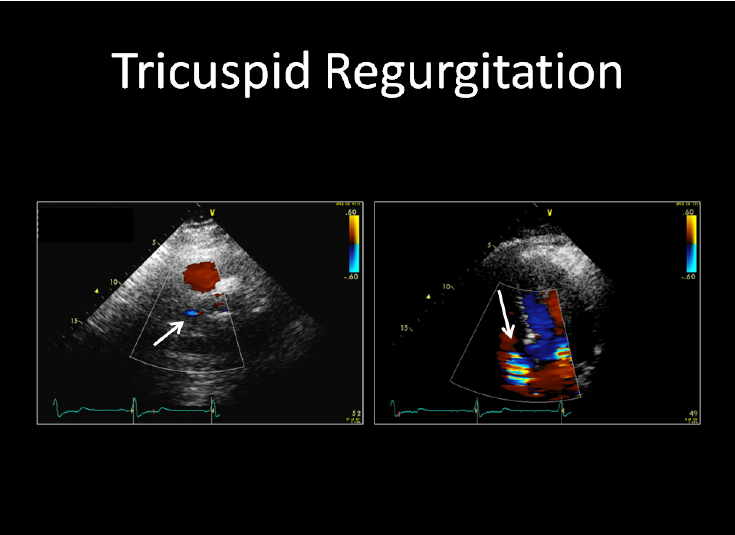
1) Tricuspid Regurgitation (TR) murmur
Definition
Backflow of blood from RV → RA during systole due to tricuspid valve incompetence.
Pathophysiology (why the murmur happens)
During systole, an incompetent valve lets blood leak back into RA → holosystolic turbulence near the tricuspid area. Inspiration increases venous return → larger regurgitant volume → louder murmur (Carvallo sign). ([MSD Manuals][1])
Causes / triggers
Most common: functional/secondary TR from RV dilation (pulmonary hypertension, left-sided HF, RV failure).
Other causes:
- Infective endocarditis (especially IVDU), rheumatic disease
- Carcinoid syndrome, congenital (Ebstein anomaly)
- Pacemaker/ICD lead-related TR, trauma, myxomatous degeneration
Murmur (core auscultation identity)
- Timing: Holosystolic (pansystolic)
- Best heard: Left lower sternal border (or epigastrium), often best with the bell; patient upright can help ([MSD Manuals][1])
- Quality/pitch: may be high-pitched if mild/PH-related; medium if severe ([MSD Manuals][1])
- Radiation: often minimal; may radiate to right sternal edge/epigastrium
- Key dynamic feature: LOUDER with inspiration (Carvallo sign) ([MSD Manuals][1])
Clinical features (what to look for with TR)
- Right HF signs: raised JVP, hepatomegaly, ascites, edema
- Pulsatile liver (hepatic systolic pulsations) can be a clue even if murmur faint ([MSD Manuals][1])
- Fatigue, abdominal fullness, RUQ discomfort
- If severe: atrial arrhythmias, cardiorenal/hepatic congestion
Investigations / diagnosis
- Echocardiography (TTE): mechanism (primary vs functional), RV size/function, TR severity, pulmonary pressures
- ECG: RA enlargement, AF/flutter
- CXR: cardiomegaly, pleural effusions
- Labs: BNP/NT-proBNP; LFTs if congestion; renal function before diuretics
Differential diagnosis (holosystolic at LLSB)
- VSD (usually harsh, often with thrill; does not increase with inspiration like TR typically does)
- MR (apex; radiates to axilla; louder expiration)
Management (stepwise)
A) Immediate/medical
- Treat cause (pulmonary hypertension, left-sided valve disease, RV infarct, device lead issue).
- Volume management (main symptomatic relief):
- Loop diuretic: Furosemide
* Indication: edema/ascites/congestion in TR/RHF
* MOA: inhibits Na-K-2Cl in thick ascending loop → natriuresis
* Typical adult dosing: 20–40 mg PO/IV; titrate (often higher in significant congestion)
* PK: onset IV ~5 min, PO 30–60 min; duration ~6 h
* Adverse effects: hypokalemia, hyponatremia, dehydration, ototoxicity (high IV doses), metabolic alkalosis
* Contraindications/cautions: severe hypovolemia, anuria (relative), sulfa allergy (caution)
* Interactions: ↑ digoxin toxicity (via low K), ↑ lithium levels, NSAIDs blunt effect
* Monitoring: weight, urine output, BP, K/Na/Mg, creatinine
* Counsel: morning dosing; report cramps/dizziness; daily weights
- Aldosterone antagonist: Spironolactone (helpful in ascites/edema, K-sparing)
* Dose (adult): 12.5–25 mg daily, titrate (often 25–50 mg/day)
* AEs: hyperkalemia, gynecomastia, menstrual irregularities
* Contraindications: hyperkalemia, severe renal failure
* Monitoring: K, creatinine within 3–7 days after start/titration
- If AF/flutter: rate control + anticoagulation per CHA₂DS₂-VASc (not TR-specific).
B) Interventional/surgical (specialist decision)
- Consider tricuspid repair (preferred) or replacement when severe symptomatic TR, progressive RV dilation/dysfunction, or when doing left-sided valve surgery (per guideline-based practice; individualized at a valve center). ([AHA Journals][3])
2) Tricuspid Stenosis (TS) murmur
Definition
Obstruction to flow RA → RV during diastole due to narrowed tricuspid valve.
Pathophysiology
Stenosis causes a diastolic pressure gradient across the valve → mid-diastolic rumble; louder with increased venous return (inspiration/leg raise/exercise). ([MSD Manuals][4])
Causes
- Rheumatic heart disease (most common worldwide) — often with MS
- Congenital, carcinoid, endocarditis/vegetations (rare), prosthetic valve dysfunction
Murmur (core auscultation identity)
- Timing: Mid-diastolic rumble with presystolic accentuation (if sinus rhythm)
- Sounds: may have a soft opening snap ([MSD Manuals][4])
- Best heard: LLSB/xiphoid area with bell, patient supine; can be subtle ([MSD Manuals][4])
- Key dynamic feature: Louder/longer with inspiration, leg raise, exercise; softer with standing/Valsalva ([MSD Manuals][4])
Clinical features
- Prominent a-wave in JVP (if sinus rhythm), fatigue
- Hepatomegaly, ascites, edema (systemic venous congestion)
- Often coexists with MS → dyspnea may be from left-sided disease
Investigations
- Echo: valve area/gradient, RA enlargement, associated MS/TR, RV function
- ECG: RA enlargement; AF common later
- Consider evaluation for rheumatic valve disease involvement
Differential diagnosis (right-sided diastolic rumble)
- Mitral stenosis (apex; louder in left lateral position; accentuated S1; OS more typical)
- Right atrial myxoma/obstructing mass (echo clarifies)
Management (stepwise)
A) Medical
- Diuretics for congestion (same agents/monitoring principles as TR)
- AF management (rate/rhythm as appropriate)
B) Anticoagulation (if AF, atrial thrombus, or rheumatic MS overlap)
- Warfarin
* Indication: AF with valvular disease where DOAC not suitable (e.g., rheumatic MS), atrial thrombus
* MOA: inhibits vitamin K-dependent clotting factors II, VII, IX, X
* Dosing: individualized; often start 2–5 mg daily and titrate
* Monitoring: INR (commonly goal 2.0–3.0 unless special indications)
* Interactions: many (amiodarone, antibiotics, antifungals, leafy greens variability)
* Counsel: consistent vitamin K intake, bleeding precautions, INR checks
C) Definitive
- Percutaneous balloon valvotomy can be considered in suitable TS anatomy (often when rheumatic and symptomatic); surgery if not suitable or combined lesions (specialist/valve-center decision).
3) Pulmonary Stenosis (PS) murmur
Definition
Obstruction to RV outflow at the pulmonary valve (or sub/supravalvular) → systolic ejection turbulence.
Pathophysiology
Narrowed outflow increases RV systolic pressure → crescendo–decrescendo ejection murmur; severity lengthens the murmur. Inspiration and Valsalva release can increase intensity. ([MSD Manuals][2])
Causes
- Congenital (most common): valvular PS (often isolated), Noonan syndrome
- Acquired: carcinoid (rare), post-surgical, RVOT obstruction variants
Murmur (core auscultation identity)
- Timing: Ejection systolic (crescendo–decrescendo)
- Best heard: Left upper sternal border (LUSB) (2nd–4th ICS) ([MSD Manuals][2])
- Radiation: typically does not radiate widely (unlike AS) ([MSD Manuals][2])
- Often associated: ejection click (may soften with inspiration in valvular PS), wide splitting of S2 (delayed P2) ([MSD Manuals][2])
- Dynamic: louder with inspiration and immediately after Valsalva release ([MSD Manuals][2])
Clinical features
- Mild: often asymptomatic
- Moderate/severe: exertional dyspnea, fatigue, syncope, angina; RV heave
- Severe longstanding: RV failure signs, cyanosis if right-to-left shunt (e.g., PFO)
Investigations
- Echo Doppler: peak gradient (severity), valve morphology, RV size/function
- ECG: RV hypertrophy
- CXR: post-stenotic dilation of main pulmonary artery (valvular PS)
Differential diagnosis (systolic ejection at LUSB)
- Innocent pulmonic flow murmur (shorter, softer, no symptoms)
- ASD (fixed split S2 + flow murmur)
- HOCM (increases with Valsalva strain, not release)
Management (stepwise)
A) Observation
- Mild, asymptomatic PS: periodic echo follow-up.
B) Definitive therapy
- Balloon pulmonary valvuloplasty is first-line for significant valvular PS (especially congenital with suitable anatomy).
- Surgery if dysplastic valve/not amenable or associated lesions.
C) Symptom/RV failure support (bridge or adjunct)
- Diuretics only if RV congestion; avoid excessive preload reduction in fixed obstruction.
4) Pulmonary Regurgitation (PR) murmur
Definition
Backflow from pulmonary artery → RV during diastole.
Pathophysiology
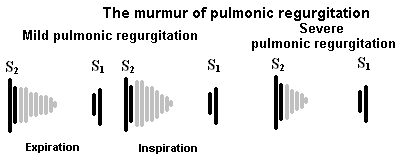
Incompetent pulmonary valve → early diastolic decrescendo murmur. If due to pulmonary hypertension, it becomes a classic high-pitched murmur beginning with P2 (Graham Steell murmur). ([MSD Manuals][5])
Causes
- Pulmonary hypertension (functional PR; classic Graham Steell) ([MSD Manuals][5])
- Post–repair of congenital heart disease (e.g., Tetralogy of Fallot)
- Infective endocarditis (rare), carcinoid, rheumatic (rare), iatrogenic
Murmur (core auscultation identity)
- Timing: Early diastolic, decrescendo
- Best heard: LUSB, diaphragm, patient sitting upright; often best at end-expiration/held breath ([MSD Manuals][5])
- Pulmonary HTN PR: high-pitched; starts with P2 and ends before S1; may radiate toward mid-right sternal edge (Graham Steell) ([MSD Manuals][5])
Clinical features
- Often silent/mild unless severe
- If severe/chronic: RV dilation → exertional dyspnea, fatigue, palpitations, RV failure signs
- In repaired congenital disease: decreased exercise tolerance, arrhythmias
Investigations
- Echo: PR severity, RV size/function, pulmonary artery pressure
- CMR can quantify RV volumes/regurgitant fraction (especially post-TOF follow-up)
- Evaluate pulmonary hypertension causes if suspected
Differential diagnosis (early diastolic decrescendo)
- Aortic regurgitation (LSB but often radiates; bounding pulse; wider pulse pressure)
- “Flow” diastolic murmurs are uncommon; diastolic murmurs are usually pathologic
Management (stepwise)
A) Treat the cause
- If pulmonary hypertension: manage the underlying etiology and consider PH-targeted therapy via specialist center. ([MSD Manuals][5])
Common PH drugs (specialist-directed; examples):
- Sildenafil (PDE-5 inhibitor): 20 mg PO TID (PAH dosing commonly used)
* AEs: headache, flushing, hypotension; contra with nitrates
- Tadalafil: 40 mg PO daily (PAH)
- Bosentan (ERA): 62.5 mg BID → 125 mg BID; monitor LFTs, teratogenic
(These require careful indication selection, hemodynamic assessment, and monitoring.)
B) Manage RV volume overload (if symptomatic)
- Loop diuretic ± spironolactone (as above); monitor renal function/electrolytes.
C) Valve intervention
- Pulmonary valve replacement (surgical or transcatheter in selected patients) when severe PR causes RV dilation/dysfunction, symptoms, or arrhythmia risk—especially common in post-congenital repair pathways.
Infective endocarditis (IE) prophylaxis (practical add-on)
Routine antibiotics are only for highest-risk cardiac conditions before certain dental procedures (not for most native valve lesions). ([www.heart.org][6])
Working external links (copy/paste)
(Placed in a code block so the URLs remain intact and clickable.)
`txt
TR (Merck/MSD Professional): https://www.msdmanuals.com/professional/cardiovascular-disorders/valvular-disorders/tricuspid-regurgitation
TS (Merck/MSD Professional): https://www.msdmanuals.com/professional/cardiovascular-disorders/valvular-disorders/tricuspid-stenosis
PS (Merck/MSD Professional): https://www.msdmanuals.com/professional/cardiovascular-disorders/valvular-disorders/pulmonary-stenosis
PR (Merck/MSD Professional): https://www.msdmanuals.com/professional/cardiovascular-disorders/valvular-disorders/pulmonary-regurgitation
Cardiac auscultation approach (Merck/MSD Professional): https://www.msdmanuals.com/professional/cardiovascular-disorders/approach-to-the-cardiac-patient/cardiac-auscultation
Rivero-Carvallo sign (TR ↑ with inspiration): https://litfl.com/rivero-carvallo-sign/
Graham Steell murmur (PR due to pulmonary HTN): https://litfl.com/graham-steell-murmur/
AHA Infective Endocarditis info: https://www.heart.org/en/health-topics/infective-endocarditis
AHA IE prophylaxis wallet card (PDF): https://www.heart.org/-/media/files/health-topics/infective-endocarditis/infective-endocarditis-wallet-card.pdf
`
If you want, I can also give a one-page “murmur differentiation table” (TS vs MS, TR vs MR/VSD, PS vs AS/flow murmur, PR vs AR) in the same no-image style.
[1]: https://www.msdmanuals.com/professional/cardiovascular-disorders/valvular-disorders/tricuspid-regurgitation?utm_source=chatgpt.com "Tricuspid Regurgitation - Cardiovascular Disorders"
[2]: https://www.msdmanuals.com/professional/cardiovascular-disorders/valvular-disorders/pulmonary-stenosis?utm_source=chatgpt.com "Pulmonary Stenosis - Cardiovascular Disorders"
[3]: https://www.ahajournals.org/doi/10.1161/CIR.0000000000000923?utm_source=chatgpt.com "2020 ACC/AHA Guideline for the Management of Patients ..."
[4]: https://www.msdmanuals.com/professional/cardiovascular-disorders/valvular-disorders/tricuspid-stenosis?utm_source=chatgpt.com "Tricuspid Stenosis - Cardiovascular Disorders"
[5]: https://www.msdmanuals.com/professional/cardiovascular-disorders/valvular-disorders/pulmonary-regurgitation?utm_source=chatgpt.com "Pulmonary Regurgitation - Cardiovascular Disorders"
[6]: https://www.heart.org/en/health-topics/infective-endocarditis?utm_source=chatgpt.com "Infective Endocarditis"
Below are 20 detailed, exam-oriented clinical case scenarios covering TS, TR, PS, and PR.
Each case includes presentation → key findings → diagnosis focus → management approach (concise but complete, as you prefer).
TRICUSPID STENOSIS (TS) – CASES
Case 1
A 45-year-old woman with a history of rheumatic fever presents with progressive fatigue, abdominal distension, and pedal edema. JVP shows prominent a-waves. Cardiac auscultation reveals a low-pitched mid-diastolic murmur at the left lower sternal border, louder with inspiration.
Diagnosis: Tricuspid stenosis
Key clue: Inspiratory accentuation + prominent a-wave
Management: Diuretics for congestion, anticoagulation if AF, evaluate for balloon valvotomy or surgery if severe.
Case 2
A patient with known rheumatic mitral stenosis develops worsening ascites and hepatomegaly despite good control of pulmonary symptoms. On auscultation, a diastolic murmur is best heard at the xiphoid area and increases with inspiration.
Diagnosis: Associated tricuspid stenosis
Key clue: MS + right-sided diastolic murmur
Management: Echo to assess valve area; treat TS if symptomatic.
Case 3
A 52-year-old woman has exertional fatigue and raised JVP with slow y-descent. ECG shows right atrial enlargement. Presystolic accentuation of a diastolic murmur disappears when she develops atrial fibrillation.
Diagnosis: Tricuspid stenosis
Key clue: Loss of presystolic accentuation in AF
Management: Rate control, anticoagulation, diuretics.
Case 4
A patient with carcinoid syndrome presents with right heart failure symptoms and a diastolic murmur at LLSB that increases with inspiration.
Diagnosis: Tricuspid stenosis (± regurgitation)
Key clue: Carcinoid preferentially affects right-sided valves
Management: Treat carcinoid + valve intervention if severe.
TRICUSPID REGURGITATION (TR) – CASES
Case 5
A 60-year-old man with dilated cardiomyopathy presents with massive pedal edema and ascites. Auscultation reveals a holosystolic murmur at LLSB that increases with inspiration.
Diagnosis: Functional tricuspid regurgitation
Key clue: Carvallo sign
Management: Diuretics, treat underlying LV failure, consider valve repair if severe.
Case 6
An IV drug user presents with fever, dyspnea, and pleuritic chest pain. Exam shows a new holosystolic murmur at LLSB and septic pulmonary emboli on imaging.
Diagnosis: Tricuspid regurgitation due to infective endocarditis
Key clue: IVDU + pulmonary septic emboli
Management: IV antibiotics, surgery if refractory or severe TR.
Case 7
A patient post-pacemaker insertion develops progressive right heart failure. Echo shows severe TR with lead impingement on the valve.
Diagnosis: Device-induced tricuspid regurgitation
Management: Diuretics, lead reposition/removal, valve repair if needed.
Case 8
A patient with long-standing pulmonary hypertension develops a pansystolic murmur at LLSB and giant v-waves in JVP.
Diagnosis: Functional tricuspid regurgitation
Key clue: Giant v-waves
Management: Treat pulmonary hypertension, manage volume overload.
Case 9
A patient with severe TR has a pulsatile liver and systolic hepatic bruit.
Diagnosis: Severe tricuspid regurgitation
Management: Aggressive diuresis, valve intervention assessment.
PULMONARY STENOSIS (PS) – CASES
Case 10
A 19-year-old woman presents with exertional dyspnea. Auscultation reveals an ejection systolic murmur at the left upper sternal border with an ejection click that decreases on inspiration.
Diagnosis: Valvular pulmonary stenosis
Management: Echo assessment; balloon valvuloplasty if moderate–severe.
Case 11
A child with Noonan syndrome presents with exertional syncope. Exam shows RV heave and systolic murmur at LUSB.
Diagnosis: Pulmonary stenosis
Key clue: Noonan syndrome association
Management: Balloon valvuloplasty or surgery.
Case 12
A patient has wide splitting of S2 with delayed P2 and a crescendo–decrescendo systolic murmur at LUSB.
Diagnosis: Pulmonary stenosis
Management: Severity assessment via Doppler gradients.
Case 13
An asymptomatic adult is found incidentally to have a mild systolic murmur at LUSB. Echo shows mild PS.
Diagnosis: Mild pulmonary stenosis
Management: Observation and periodic follow-up only.
Case 14
A patient with severe PS develops exertional angina and syncope.
Diagnosis: Critical pulmonary stenosis
Mechanism: Fixed RV outflow obstruction → limited CO
Management: Urgent intervention.
PULMONARY REGURGITATION (PR) – CASES
Case 15
A patient with long-standing pulmonary hypertension develops a high-pitched early diastolic murmur at LUSB starting immediately after P2.
Diagnosis: Graham Steell murmur (PR due to PH)
Management: Treat pulmonary hypertension.
Case 16
A 28-year-old patient status post Tetralogy of Fallot repair presents with declining exercise tolerance. A decrescendo early diastolic murmur is heard at LUSB.
Diagnosis: Chronic pulmonary regurgitation
Management: Monitor RV size; pulmonary valve replacement if RV dilation.
Case 17
A patient with severe PR develops progressive RV dilation and ventricular arrhythmias.
Diagnosis: Severe pulmonary regurgitation
Management: Pulmonary valve replacement.
Case 18
A diastolic murmur at LUSB becomes louder with inspiration and is blowing in nature.
Diagnosis: Pulmonary regurgitation
Management: Echo to identify etiology (PH vs post-surgical).
MIXED / DIFFERENTIATION CASES
Case 19
A diastolic murmur is heard at LLSB and apex. The murmur increases with inspiration and decreases during expiration.
Diagnosis: Tricuspid stenosis (not mitral stenosis)
Key differentiation: Respiratory variation.
Case 20
A holosystolic murmur at LLSB is suspected to be VSD. However, murmur intensity increases with inspiration and there is no thrill.
Diagnosis: Tricuspid regurgitation
Key differentiation: Carvallo sign, absence of thrill.