Definition
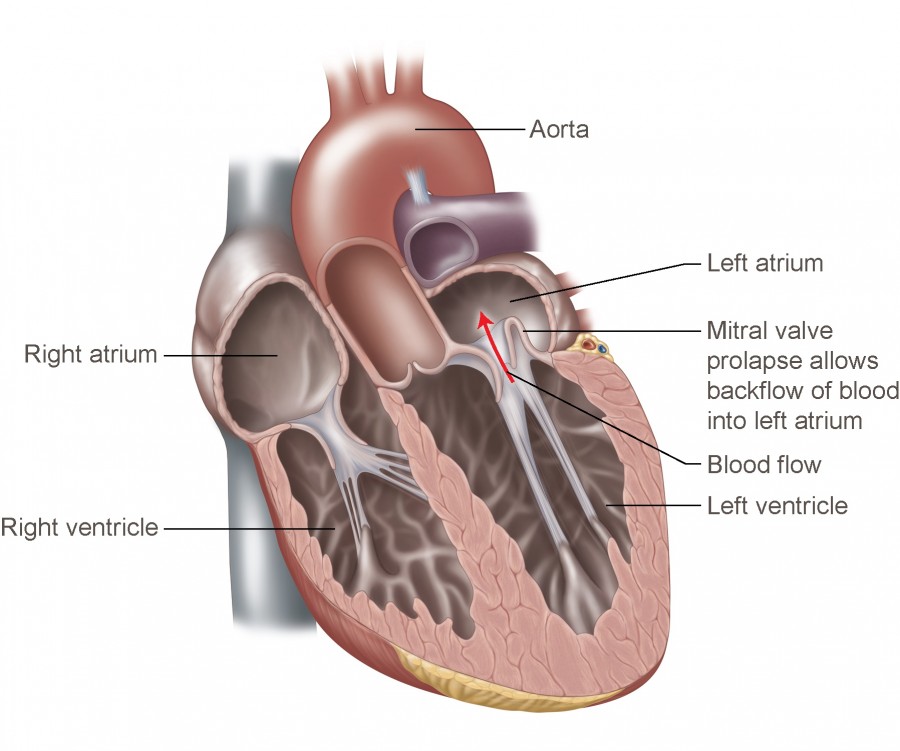
Mitral valve prolapse is a myxomatous degeneration of the mitral valve in which one or both mitral leaflets billow ≥2 mm into the left atrium during systole, sometimes causing mitral regurgitation (MR).
Epidemiology
- Prevalence: ~2–3% of general population
- More common in women, often detected in young to middle age
- Usually benign, but a subset develops complications
Pathophysiology
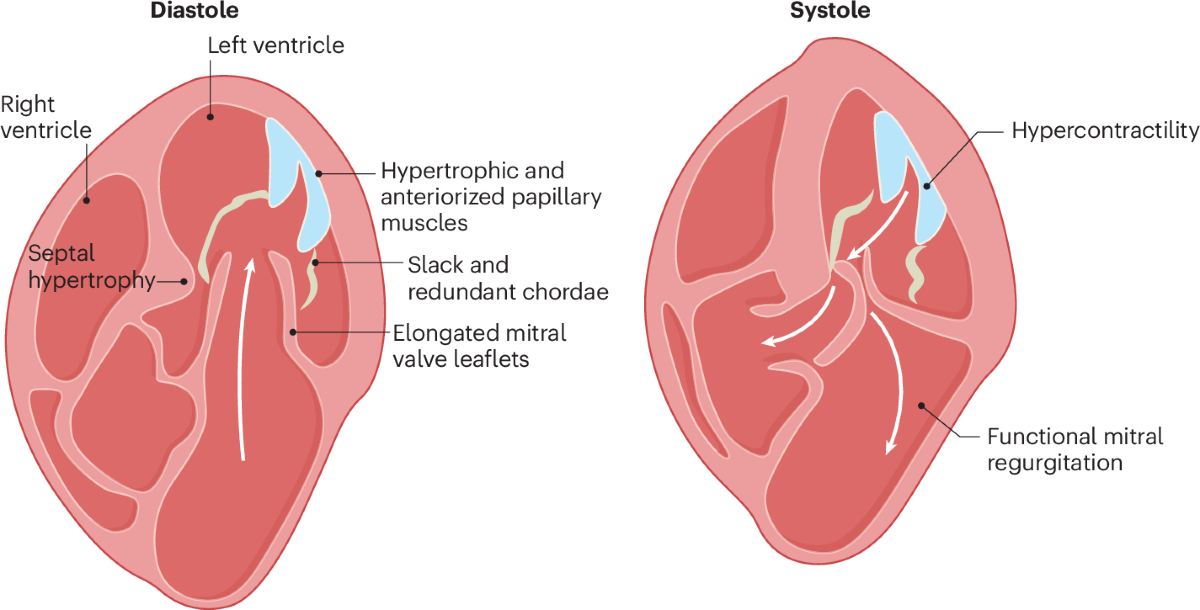
- Myxomatous degeneration → leaflet thickening, redundancy
- Elongation/rupture of chordae tendineae
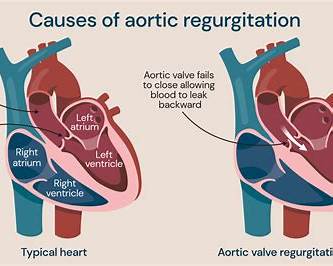
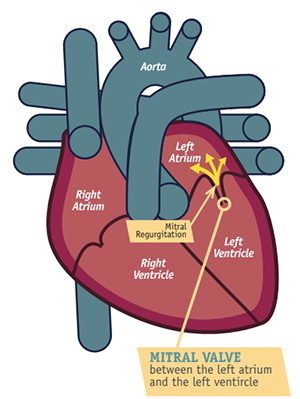
- Incomplete leaflet coaptation → mitral regurgitation
- Abnormal tension on papillary muscles → chest pain, arrhythmias
Etiology / Associations
- Primary (Idiopathic) – most common
- Connective tissue disorders:
* Marfan syndrome
* Ehlers–Danlos syndrome
- Secondary MVP:
* Ischemic heart disease
* Rheumatic heart disease
* Hypertrophic cardiomyopathy
- Familial (autosomal dominant inheritance reported)
Clinical Features
Asymptomatic (most common)
- Incidentally detected murmur or echo finding
Symptomatic
- Palpitations (due to atrial or ventricular ectopics)
- Atypical chest pain (non-exertional, sharp)
- Dyspnea, fatigue
- Anxiety, panic symptoms
- Dizziness, syncope (rare)
Physical Examination
- Mid-systolic click (due to sudden tensing of chordae)
- Late systolic murmur at apex (if MR present)
- Murmur moves earlier and becomes louder with:
* Standing
* Valsalva maneuver
- Murmur moves later and softens with:
* Squatting
* Handgrip
Investigations
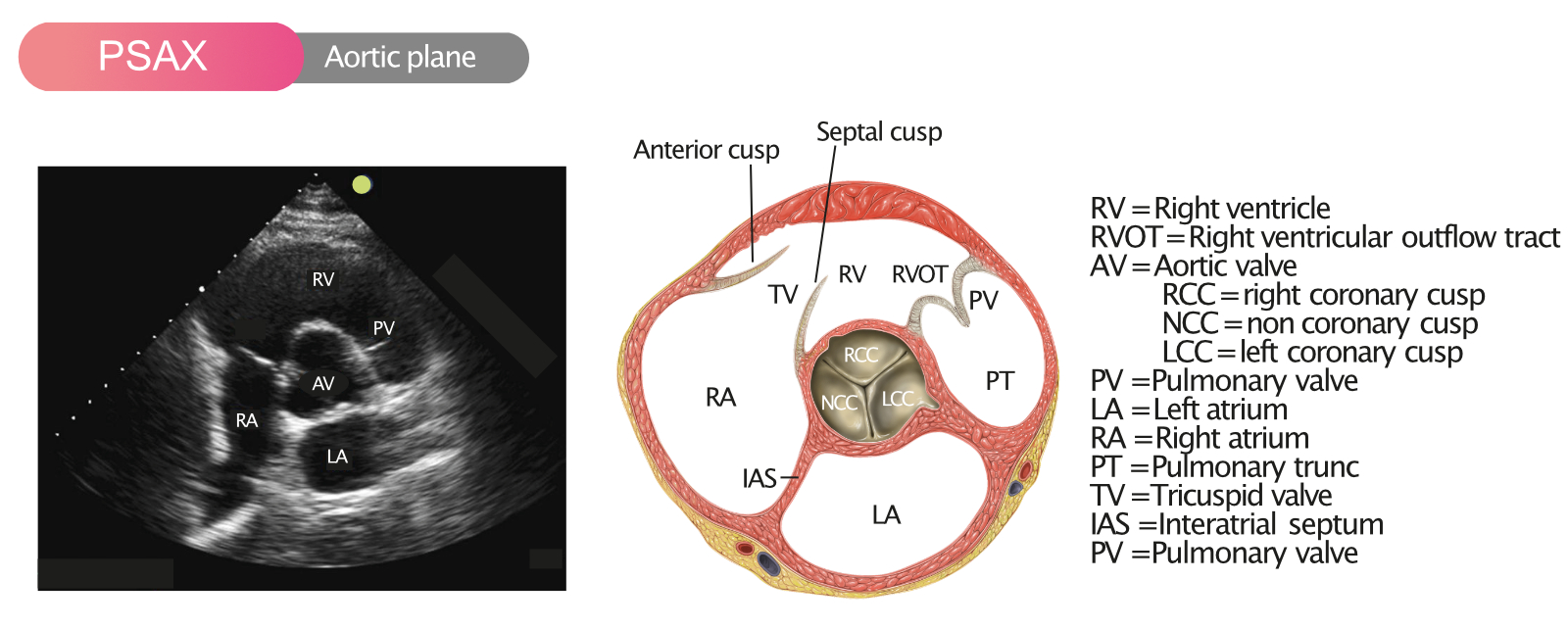
1. Echocardiography (Gold Standard)
- Leaflet displacement ≥2 mm into LA in systole
- Assess:
* Leaflet thickness (>5 mm suggests myxomatous MVP)
* Degree of mitral regurgitation
* LV size and function
* Chordal rupture
2. ECG
- Often normal
- May show:
* PVCs
* Non-specific ST–T changes
3. Holter Monitoring
- For palpitations or syncope
- Detects ventricular arrhythmias
4. Chest X-ray
- Usually normal
- LA/LV enlargement if significant MR
Differential Diagnosis
- Mitral regurgitation (other causes)
- Hypertrophic cardiomyopathy
- Atrial septal defect
- Tricuspid valve prolapse
- Functional systolic murmurs
Complications
- Progressive mitral regurgitation
- Infective endocarditis
- Arrhythmias (atrial fibrillation, ventricular ectopy)
- Stroke / TIA (rare)
- Sudden cardiac death (very rare, high-risk subset)
Management
Asymptomatic MVP (No MR or Mild MR)
- Reassurance
- Periodic follow-up (echo every 3–5 years)
- No activity restriction
Symptomatic MVP (Palpitations, Chest Pain)
Beta-blockers (First line)
- Indication: Palpitations, anxiety, chest pain
- Mechanism: Reduce sympathetic tone, suppress ectopy
- Examples & Dosing:
* Propranolol: 10–40 mg PO 2–3×/day
* Metoprolol: 25–100 mg/day
- Adverse effects: Bradycardia, fatigue
- Contraindications: Asthma, severe bradycardia
MVP With Mitral Regurgitation
Medical
- ACE inhibitors (if LV dysfunction)
- Diuretics (if pulmonary congestion)
- Rate/rhythm control if AF develops
Surgical (Mitral Valve Repair Preferred)
Indications
- Severe MR with symptoms
- Severe MR + LV dysfunction
* LVEF ≤60%
* LVESD ≥40 mm
- New-onset atrial fibrillation
- Pulmonary hypertension
Infective Endocarditis Prophylaxis
- Not routinely recommended
- Only for:
* Prior infective endocarditis
* Prosthetic valve
* Certain congenital heart diseases
Lifestyle & Counseling
- Avoid excessive caffeine and stimulants
- Regular aerobic exercise (if no severe MR)
- Reassure regarding benign nature in most cases
- Educate about symptoms of worsening MR (dyspnea, edema)
Prognosis
- Excellent in majority without significant MR
- Risk increases with:
* Thickened leaflets
* Severe MR
* Ventricular arrhythmias
- Lifelong follow-up required if MR present