1) Definition
Symptomatic bradycardia with a pulse — heart rate low enough to cause symptoms (usually <60 bpm, commonly <50–40 bpm depending on context) and the patient has a palpable pulse and circulation but shows signs of inadequate tissue perfusion (syncope, presyncope, hypotension, altered mental status, ischemic chest pain, acute heart failure). ([Cleveland Clinic][1])
2) Pathophysiology (brief)
Slow heart rate reduces cardiac output (CO ≈ HR × stroke volume). If compensatory mechanisms (increased stroke volume, peripheral vasoconstriction) fail, cerebral and coronary perfusion falls → syncope, dizziness, chest pain, hypotension, shock. Causes of impaired impulse generation (sinus node dysfunction) or impulse conduction (AV block) produce bradycardia. ([American Heart Association Journals][2])
3) Common causes & triggers
- Intrinsic cardiac — sick sinus syndrome, AV block (Mobitz II, 3rd degree), ischemia/infarction (especially inferior MI), conduction system disease. ([American Heart Association Journals][2])
- Drugs — β-blockers, non-dihydropyridine Ca-channel blockers (verapamil, diltiazem), digoxin, antiarrhythmics (eg, amiodarone), clonidine, opioid overdose. ([Cleveland Clinic][1])
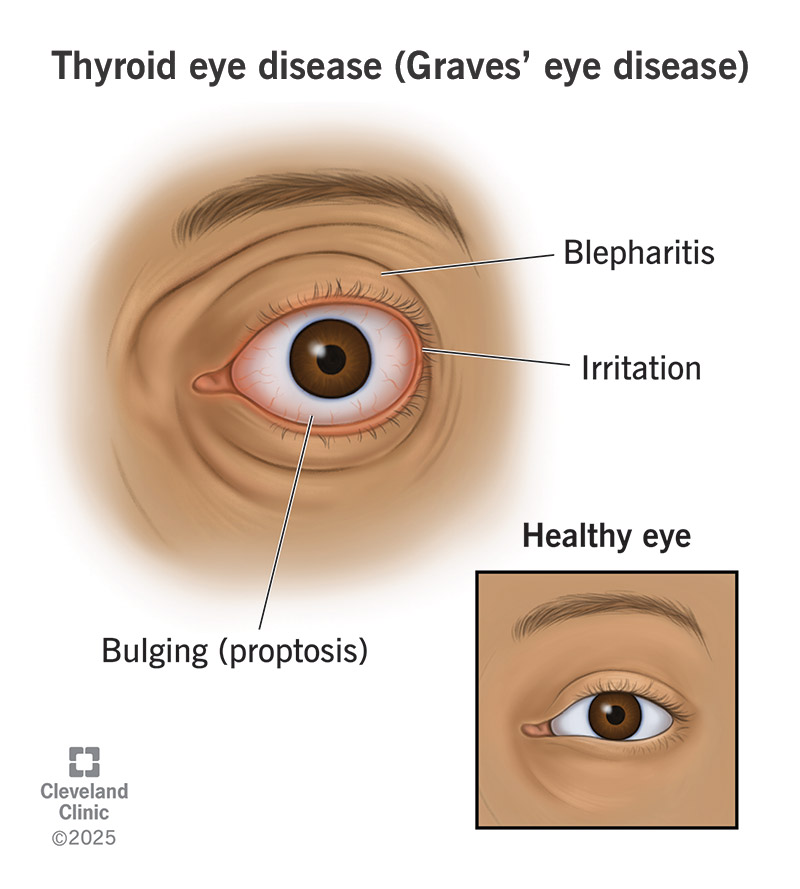
- Metabolic / toxic — hyperkalemia, hypothyroidism, severe hypothermia, organophosphate poisoning. ([Mayo Clinic][3])
- Hypoxia, severe vagal stimulation, increased intracranial pressure, athletic high vagal tone (often asymptomatic). ([Cleveland Clinic][1])
4) Clinical features (symptoms & signs)
Symptoms related to low cerebral/coronary perfusion: syncope or presyncope, lightheadedness, weakness, fatigue, confusion, dyspnea, chest pain, diaphoresis. Signs: bradycardia on monitor/ECG, hypotension, cool clammy skin if shocky, reduced level of consciousness if severe. ([Mayo Clinic][3])
5) Immediate assessment (ABC & focused)
- Airway / breathing / oxygenation. Give oxygen if hypoxic.
- Continuous cardiac monitoring, pulse oximetry, BP measurement, IV/IO access.
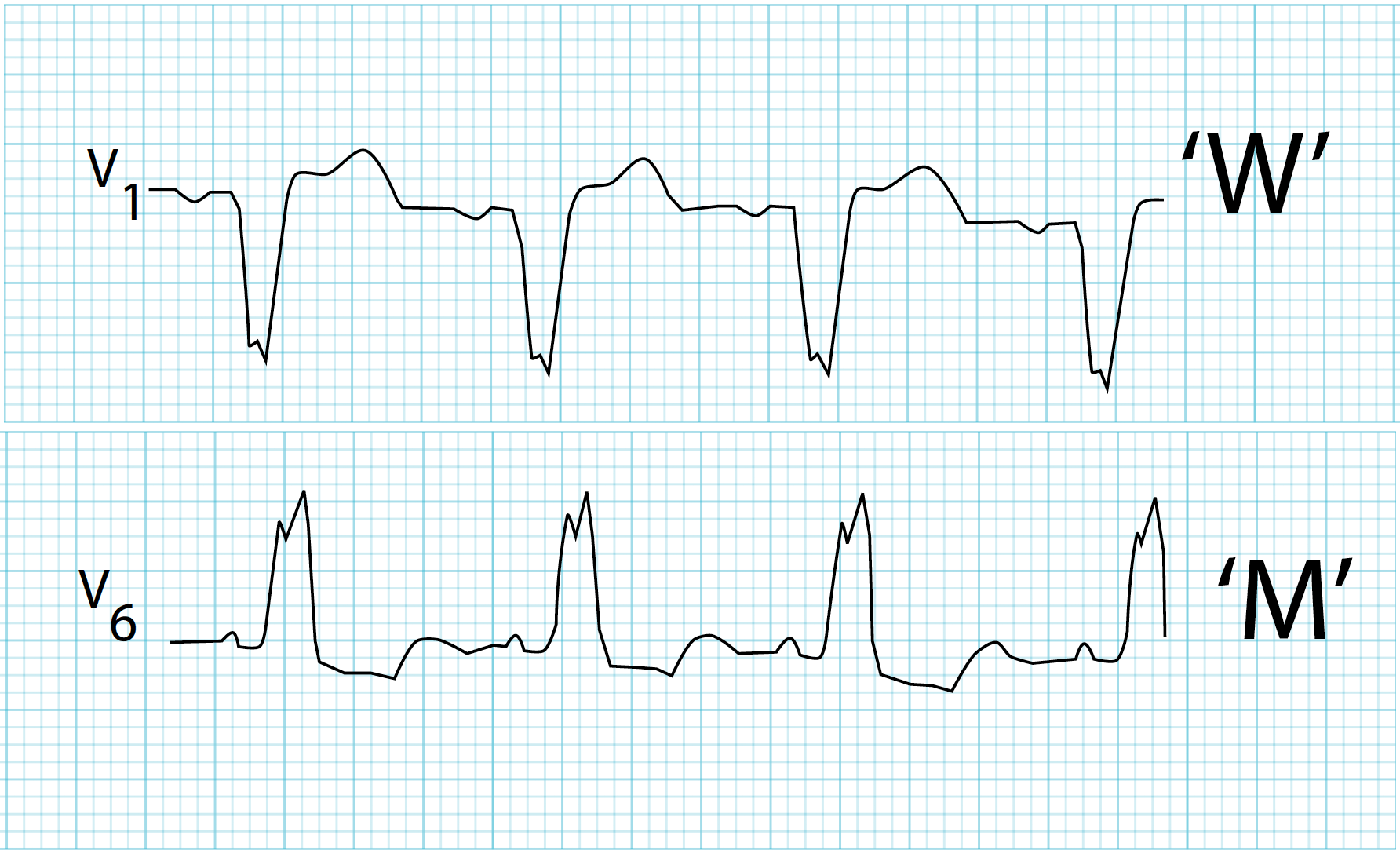
- 12-lead ECG ASAP to identify rhythm (sinus bradycardia vs AV block vs pause vs junctional rhythm).
- Rapid history for drugs, recent MI, prodrome, chronic conduction disease, comorbidities.
- Point-of-care glucose, electrolytes (K+, Mg2+), thyroid tests, troponin if ischemia suspected. ([cpr.heart.org][4])
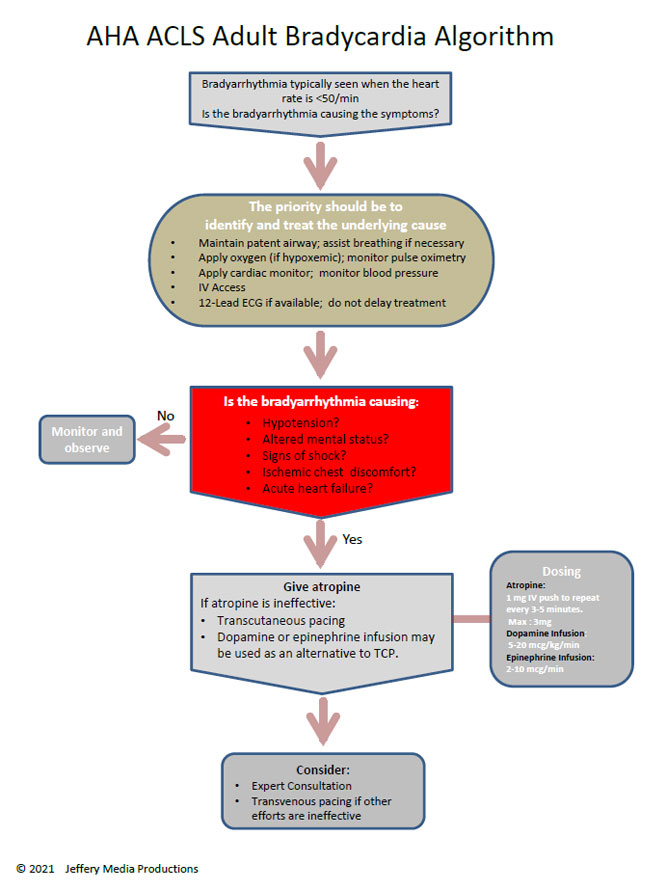
6) Stepwise management (practical algorithm — adult)
> This follows standard ACLS/Adult Bradycardia with a Pulse algorithm (initial stabilization → atropine → consider chronotropic infusions or pacing) and then definitive therapy if persistent. See official algorithm pdf. ([cpr.heart.org][4])
A. Immediate resuscitation / unstable patient
If signs of severe instability (hypotension, shock, ischemic chest pain, acute altered mental status, severe heart failure) → treat immediately:
- Call for help / expert (cardiology, electrophysiology).
- Prepare for immediate transcutaneous pacing (TCP) AND/OR consider vasopressor infusion if TCP not available or ineffective. Start oxygen and IV fluids if hypovolemic. ([cpr.heart.org][4])
B. Pharmacologic steps (if patient has a pulse and is symptomatic but not in cardiac arrest)
- Atropine — first-line IV agent to attempt to increase heart rate.
Adult dose (per most recent ACLS algorithm): 1 mg IV bolus; repeat every 3–5 minutes as needed; maximum total 3 mg. (Note: older references list 0.5 mg initial — check local ACLS protocol; many recent algorithm documents show 1 mg as initial bolus.)* ([cpr.heart.org][4])
- If atropine ineffective or insufficient / if high-degree AV block or anticipated poor response — choose one:
* Transcutaneous pacing (TCP) — apply pads and begin pacing at lowest energy needed to capture; provide analgesia/sedation as able. Prepare for transvenous pacing if prolonged requirement. ([cpr.heart.org][4])
* OR chronotropic infusion if pacing not immediately available or as adjunct:
* Dopamine infusion: typically 5–20 µg/kg/min, titrate to effect (some protocols use 2–10 µg/kg/min or 5–20). ([cpr.heart.org][4])
* Epinephrine infusion: 2–10 µg/min infusion titrated to effect (some protocols use µg/kg/min in arrest; for bradycardia infusion use µg/min). ([cpr.heart.org][4])
- If drug overdose (eg β-blocker or Ca-channel blocker) suspected: specific therapy (IV glucagon for beta-blocker, high-dose insulin/euglycemia therapy and calcium for severe Ca-channel blocker overdose) and urgent cardiology/toxicology consult. ([Cleveland Clinic][1])
C. Ongoing care / escalation
- If persistent symptomatic bradycardia not responsive to above → transvenous pacing or consideration of permanent pacemaker (see indications). Consult electrophysiology/cardiology early. ([European Society of Cardiology][5])
7) Drugs — indication, mechanism, dosing, monitoring, adverse effects, cautions
> Below I give the clinically most used agents for adult symptomatic bradycardia. For paediatric doses see PALS (short summary below and PALS pdf link). ([cpr.heart.org][6])
Atropine
- Indication: Symptomatic bradycardia (to increase heart rate by inhibiting vagal tone). ([cpr.heart.org][4])
- Mechanism: Antimuscarinic (blocks M2 receptors in SA/AV nodes) → decreases vagal influence → ↑ HR.
- Adult dosing: 1 mg IV bolus (many ACLS docs state 1 mg initial), repeat every 3–5 min, max 3 mg total. (Older guidance: 0.5 mg initial — check local protocol.) ([cpr.heart.org][4])
- Pediatric dosing (PALS): 0.02 mg/kg IV (minimum single dose 0.1 mg; maximum single dose 0.5 mg for infants and 1 mg for adolescents); may repeat once. See PALS guidelines for full details. ([cpr.heart.org][6])
- Onset/duration (PK): Rapid onset IV (minutes); duration variable (30–60 min).
- Common adverse effects: Dry mouth, blurred vision, tachycardia, urinary retention, agitation.
- Serious risks: May worsen ischemia in acute MI by increasing HR and oxygen demand; may worsen conduction in infra-Hisian block sometimes (paradoxical bradycardia in high doses).
- Contraindications / interactions: Use caution in glaucoma, prostatic hypertrophy; interacts with other anticholinergics.
- Monitoring: Continuous ECG, BP, mental status. ([cpr.heart.org][4])
Dopamine (infusion)
- Indication: Symptomatic bradycardia refractory to atropine or when pacing not feasible. ([cpr.heart.org][4])
- Mechanism: Dose-dependent: low doses vasodilation (renal), moderate β-agonist effect (↑HR/contractility), high α-agonist vasoconstriction. In bradycardia used for positive chronotropic and inotropic effect.
- Adult dosing: 5–20 µg/kg/min (titrate to hemodynamic response). Some local protocols use 2–10 µg/kg/min — follow local formulary. ([cpr.heart.org][4])
- Onset/duration: Rapid onset IV infusion; short half-life.
- Adverse effects: Tachyarrhythmias, hypertension, ischemia, extravasation risk (use central line if possible).
- Monitoring: Continuous ECG, BP, urine output, infusion site. ([cpr.heart.org][4])
Epinephrine (infusion)
- Indication: Alternative chronotrope/pressor when atropine ineffective. ([cpr.heart.org][4])
- Mechanism: α and β adrenergic agonist → ↑ HR and peripheral vascular resistance.
- Adult dosing (infusion for bradycardia): 2–10 µg/min infusion, titrate to effect (some ACLS texts describe ranges). In arrest, bolus dosing differs. ([cpr.heart.org][4])
- Adverse effects: Tachyarrhythmia, hypertension, myocardial ischemia, hyperglycemia, lactic acidosis.
- Monitoring: ECG, BP, end-organ perfusion. ([cpr.heart.org][4])
8) Pacing (temporary & permanent) — when and how
Transcutaneous pacing (TCP)
- Rapid temporary measure when bradycardia causes instability and drugs ineffective/contraindicated. Apply pads, set rate (eg 60–80 bpm) and increase current until electrical capture and then confirm mechanical capture (palpable pulse, BP improvement). Provide analgesia/sedation if patient conscious. Prepare for transvenous or permanent pacing if pacing required > short term. ([cpr.heart.org][4])
Transvenous (temporary) pacing
- Placed by trained operator if prolonged temporary pacing needed or TCP cannot be tolerated/ineffective. ([European Society of Cardiology][5])
Permanent pacemaker — indications (representative):
- Symptomatic sinus node dysfunction (sick sinus) causing syncope or symptomatic bradycardia not correctable by reversible causes; high-grade AV block (Mobitz II or third-degree) not expected to resolve; bradycardia producing heart failure or chronotropic incompetence. Follow ACC/AHA/HRS guideline for detailed class recommendations. ([HRS][7])
9) Differential diagnoses to consider
- Vasovagal syncope (may have transient bradycardia)
- Seizure/post-ictal state (may cause transient bradycardia)
- Hypoglycaemia (can mimic dizziness/syncope)
- Orthostatic hypotension
- Drug overdose / intoxication (opioids, clonidine, beta-blockers)
- Sinus arrest vs AV block vs junctional escape rhythms on ECG — ECG distinguishes. ([Mayo Clinic][3])
10) Investigations / workup after initial stabilization
- 12-lead ECG (identify rhythm, AV block level, ischemia).
- Continuous telemetry / telemetry unit.
- Serum electrolytes (K+, Mg2+, Ca2+), renal function, glucose, TSH.
- Cardiac biomarkers (troponin) if ischemia suspected.
- Drug levels where appropriate (digoxin).
- Chest X-ray if cardiomegaly/lead placement planning.
- Consider echocardiography to evaluate structural heart disease. ([Mayo Clinic][3])
11) Disposition & follow-up
- Admit to monitored bed (telemetry/ICU depending on severity).
- Cardiology/electrophysiology consult for persistent bradycardia, recurrent syncope, high-grade AV block, or if permanent pacing may be indicated. ([HRS][7])
12) Patient counselling (brief)
- Explain cause if known (drug effect, conduction disease, MI). Don’t stop medications (eg β-blocker) without physician advice. If a pacemaker is required, explain procedure, risks, and follow-up. Educate on symptoms that need urgent review (syncope, chest pain, severe dizziness). ([Mayo Clinic][3])
13) Pediatric notes (very brief)
- PALS guidance differs: in symptomatic bradycardia with poor perfusion due to hypoxia or shock, treat underlying cause first and use epinephrine (0.01 mg/kg IV) and atropine dosing per PALS. See PALS bradycardia algorithm for full pediatric dosing and nuances. ([cpr.heart.org][6])
14) Quick reference summary (one-line actions)
- Airway, breathing, oxygen, IV access, monitor, 12-lead ECG.
- If unstable → immediate TCP and call cardiology; consider epinephrine/dopamine infusion.
- If stable but symptomatic → atropine 1 mg IV q3–5 min up to 3 mg; if no response, TCP or dopamine/epinephrine infusion.
- Investigate reversible causes (drugs, electrolytes, ischemia).
- If persistent → transvenous pacing / evaluate for permanent pacemaker. ([cpr.heart.org][4])
15) Key references / external links (authoritative)
- AHA / ACLS Adult Bradycardia with Pulse Algorithm (official PDF) — recommended algorithm & drug doses. ([cpr.heart.org][4])
- Cleveland Clinic — Bradycardia: Symptoms, Causes & Treatment. Good patient-oriented overview. ([Cleveland Clinic][1])
- Mayo Clinic — Bradycardia: Diagnosis and treatment. Practical clinician/patient info. ([Mayo Clinic][3])
- ESC Guidelines — Cardiac pacing (2021) — pacing indications and device therapy context. ([European Society of Cardiology][5])
- 2018 ACC/AHA/HRS Guideline — detailed indications for pacing and evaluation of bradyarrhythmias. ([American Heart Association Journals][2])
If you want, I can now:
- Convert this into a single-page printable handout (PDF) for ER use; OR
- Produce ACLS-style pocket cards (small digest of doses/steps) as HTML you can print; OR
- Make a differential + 30 case-scenario set with stepwise management (useful for teaching / MCQs) — say which you prefer and I’ll produce it right away.
Which of those would be most helpful?
[1]: https://my.clevelandclinic.org/health/diseases/17841-bradycardia?utm_source=chatgpt.com "Bradycardia: Symptoms, Causes & Treatment"
[2]: https://www.ahajournals.org/doi/10.1161/CIR.0000000000000628?utm_source=chatgpt.com "2018 ACC/AHA/HRS Guideline on the Evaluation and ..."
[3]: https://www.mayoclinic.org/diseases-conditions/bradycardia/symptoms-causes/syc-20355474?utm_source=chatgpt.com "Bradycardia - Symptoms and causes"
[4]: https://cpr.heart.org/-/media/CPR-Files/CPR-Guidelines-Files/2025-Algorithms/Algorithm-ACLS-Bradycardia-250514.pdf?sc_lang=en&utm_source=chatgpt.com "Adult Bradycardia With a Pulse Algorithm"
[5]: https://www.escardio.org/Guidelines/Clinical-Practice-Guidelines/Cardiac-Pacing-and-Cardiac-Resynchronization-Therapy?utm_source=chatgpt.com "2021 ESC Guidelines on cardiac pacing and ..."
[6]: https://cpr.heart.org/-/media/cpr-files/cpr-guidelines-files/algorithms/algorithmpals_bradycardia_200707.pdf?la=en&utm_source=chatgpt.com "Pediatric Bradycardia With a Pulse Algorithm"
[7]: https://www.hrsonline.org/wp-content/uploads/2025/02/2018-ACC-AHA-HRS-Bradycardia_ES.pdf?ref%253Dtomba.io=&utm_source=chatgpt.com "2018 ACC/AHA/HRS guideline on the evaluation and ..."
Below is a comprehensive, exam-oriented and clinical reference covering 30 detailed differential case scenarios of symptomatic bradycardia with pulse, each with focused management and key contraindications.
Structured for ER, ICU, cardiology teaching, and MCQ/case-based learning.
SYMPTOMATIC BRADYCARDIA WITH PULSE
30 DIFFERENTIAL CASE SCENARIOS WITH DETAILED MANAGEMENT AND CONTRAINDICATIONS
1. Sinus Bradycardia due to Beta-Blocker Excess
Case: HR 38/min, dizziness, on metoprolol
Management:
- Stop beta-blocker
- Atropine IV if symptomatic
- IV glucagon in overdose
Contraindications:
- Avoid calcium channel blockers
- Avoid additional beta-blockers
2. Calcium Channel Blocker Toxicity
Case: Bradycardia, hypotension, verapamil use
Management:
- IV calcium gluconate
- High-dose insulin euglycemia therapy
- Atropine (often ineffective)
Contraindications:
- Avoid beta-blockers
- Avoid adenosine
3. Digoxin Toxicity
Case: HR 32/min, nausea, yellow vision
Management:
- Stop digoxin
- Digoxin-specific Fab antibodies
- Correct electrolytes
Contraindications:
- Avoid calcium
- Avoid cardioversion unless unstable
4. Inferior Wall Myocardial Infarction
Case: Bradycardia, hypotension, nausea
Management:
- Atropine first-line
- IV fluids
- Temporary pacing if refractory
Contraindications:
- Avoid beta-blockers acutely
- Avoid nitrates if RV involvement
5. Right Ventricular Infarction
Case: Bradycardia, raised JVP, hypotension
Management:
- IV fluids
- Atropine
- Pacing if needed
Contraindications:
- Avoid nitrates
- Avoid diuretics
6. Sick Sinus Syndrome
Case: Sinus pauses, syncope
Management:
- Temporary pacing if unstable
- Permanent pacemaker (definitive)
Contraindications:
- Avoid beta-blockers
- Avoid non-DHP calcium blockers
7. Mobitz Type II AV Block
Case: Sudden dropped QRS, HR 40
Management:
- Immediate pacing
- Permanent pacemaker
Contraindications:
- Avoid atropine reliance
- Avoid AV-node blocking drugs
8. Complete Heart Block
Case: HR 28/min, hypotension, syncope
Management:
- Transcutaneous pacing
- Transvenous pacing
- Permanent pacemaker
Contraindications:
- Atropine often ineffective
- Avoid discharge without pacing
9. Hyperkalemia-Induced Bradycardia
Case: HR 35/min, wide QRS
Management:
- IV calcium gluconate
- Insulin + glucose
- Dialysis if severe
Contraindications:
- Avoid beta-blockers
- Avoid potassium-sparing diuretics
10. Hypothyroidism
Case: Bradycardia, weight gain, cold intolerance
Management:
- Thyroxine replacement
- Supportive care
Contraindications:
- Avoid rapid IV thyroxine unless myxedema coma
11. Hypothermia
Case: HR 30/min, temp 32°C
Management:
- Active rewarming
- Gentle handling
Contraindications:
- Avoid atropine (ineffective)
- Avoid pacing unless unstable
12. Vasovagal Syncope
Case: Bradycardia after pain/emotion
Management:
- Supine positioning
- IV fluids
- Atropine if recurrent
Contraindications:
- Avoid unnecessary pacing
13. Carotid Sinus Hypersensitivity
Case: Syncope on neck turning
Management:
- Avoid triggers
- Pacemaker if recurrent
Contraindications:
- Avoid carotid massage in stroke risk
14. Raised Intracranial Pressure
Case: Bradycardia + hypertension
Management:
- Treat intracranial cause
- Mannitol, ventilation
Contraindications:
- Avoid atropine as sole therapy
15. Sepsis with Relative Bradycardia
Case: Fever with low HR
Management:
- Treat sepsis
- Fluids, antibiotics
Contraindications:
- Avoid pacing unless shock
16. Athletic Bradycardia
Case: HR 35/min, asymptomatic
Management:
- No treatment
Contraindications:
- Avoid atropine
- Avoid pacemaker
17. Post-Cardiac Surgery Bradycardia
Case: Bradycardia after valve surgery
Management:
- Temporary pacing wires
- Observe 5–7 days
Contraindications:
- Avoid premature permanent pacing
18. Drug-Induced AV Block (Amiodarone)
Case: HR 40/min on amiodarone
Management:
- Stop drug
- Temporary pacing if needed
Contraindications:
- Avoid re-challenge
19. Opioid Overdose
Case: Bradycardia, pinpoint pupils
Management:
- Naloxone
- Airway support
Contraindications:
- Avoid atropine as primary treatment
20. Organophosphate Poisoning
Case: Bradycardia, salivation, sweating
Management:
- Atropine (high dose)
- Pralidoxime
Contraindications:
- Avoid beta-blockers
21. Myxedema Coma
Case: Severe hypothyroidism, bradycardia
Management:
- IV levothyroxine
- Hydrocortisone
Contraindications:
- Avoid sedatives
22. Lyme Carditis
Case: Young patient, AV block, tick exposure
Management:
- IV antibiotics
- Temporary pacing
Contraindications:
- Avoid permanent pacemaker initially
23. Sarcoidosis-Related AV Block
Case: Young adult with heart block
Management:
- Steroids
- Permanent pacemaker/ICD
Contraindications:
- Avoid observation alone
24. Post-MI Ventricular Septal Rupture
Case: Bradycardia with shock
Management:
- Emergency surgery
- Temporary pacing
Contraindications:
- Avoid delay
25. Bradycardia in Pregnancy
Case: HR 40/min, asymptomatic
Management:
- Observe
- Treat cause
Contraindications:
- Avoid unnecessary drugs
26. Bradycardia from Increased Vagal Tone (Sleep)
Case: Night-time bradycardia
Management:
- Reassurance
Contraindications:
- Avoid pacing
27. Electrolyte Disturbance (Hypokalemia)
Case: Bradycardia with U waves
Management:
- Potassium replacement
Contraindications:
- Avoid digoxin
28. Acute Aortic Dissection
Case: Bradycardia with hypotension
Management:
- Emergency surgery
- BP control
Contraindications:
- Avoid anticoagulation
29. Pacemaker Failure
Case: Known pacemaker, bradycardia
Management:
- Magnet application
- Device interrogation
Contraindications:
- Avoid discharge without fix
30. Chronotropic Incompetence
Case: Exertional syncope, HR fails to rise
Management:
- Permanent pacemaker
Contraindications:
- Avoid beta-blockers