**Advanced Cardiac Life Support (ACLS)
Advanced Cardiac Life Support (ACLS) is a set of evidence-based clinical algorithms developed to manage adult cardiac arrest, peri-arrest conditions, and life-threatening cardiovascular emergencies. It builds upon Basic Life Support (BLS) and emphasizes high-quality CPR, early defibrillation, advanced airway management, pharmacology, and team-based resuscitation.
1. Goals of ACLS
- Restore spontaneous circulation (ROSC)
- Optimize oxygenation and perfusion
- Identify and treat reversible causes
- Minimize neurological injury
- Improve survival with good neurological outcome
2. Core Principles of ACLS
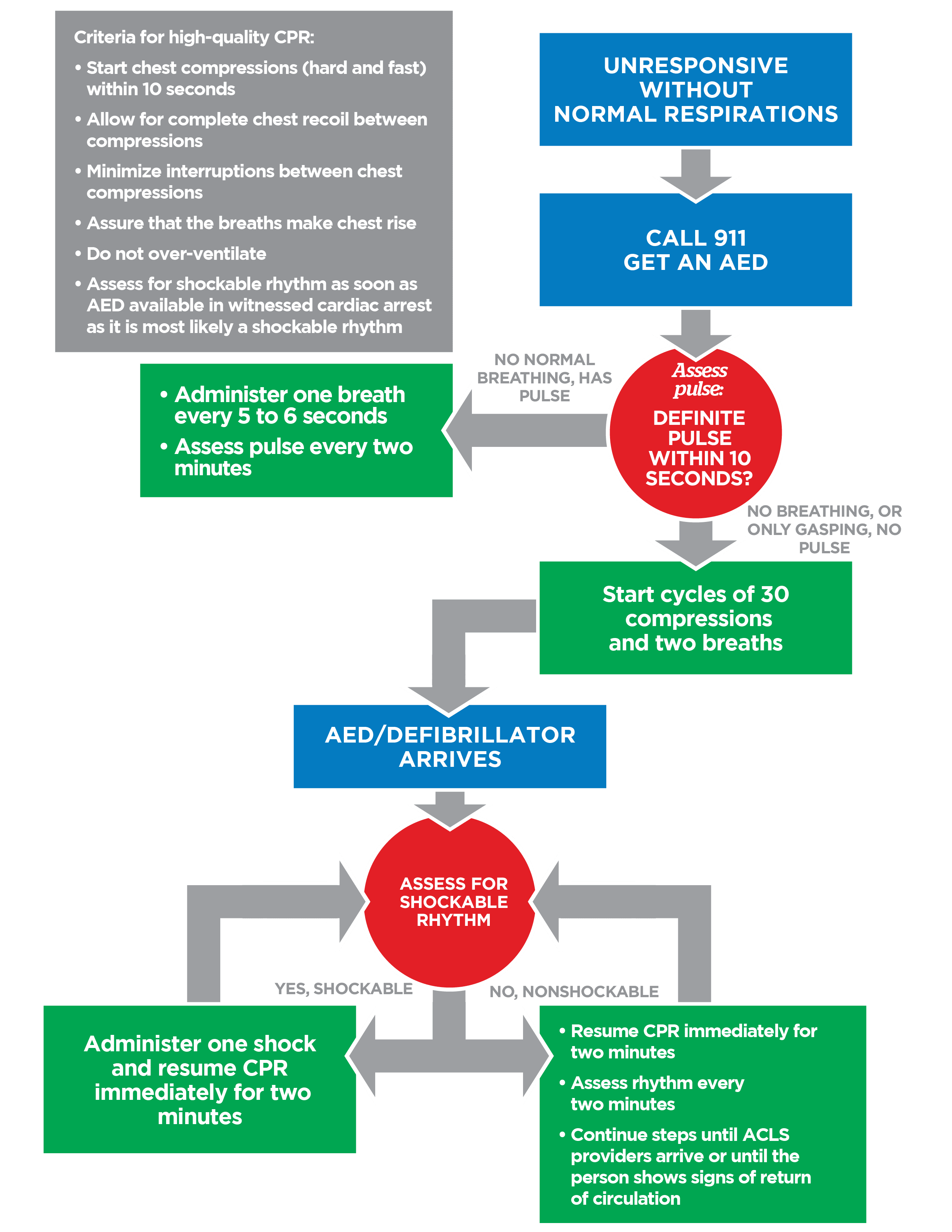
High-Quality CPR
- Rate: 100–120/min
- Depth: 5–6 cm (2–2.4 inches)
- Full chest recoil
- Minimize interruptions (<10 seconds)
- Compression-to-ventilation ratio:
* 30:2 (no advanced airway)
* Continuous compressions + 1 breath every 6 sec (advanced airway)
Early Defibrillation
- Most effective for VF/pVT
- Biphasic: 120–200 J
- Monophasic: 360 J
Airway and Ventilation
- Oxygen initially; titrate to SpO₂ 94–99% after ROSC
- Advanced airway:
* Endotracheal tube
* Supraglottic airway
- Confirm placement with capnography
* CPR quality marker: ETCO₂ ≥10 mmHg
* ROSC indicator: sudden ETCO₂ rise (>40 mmHg)
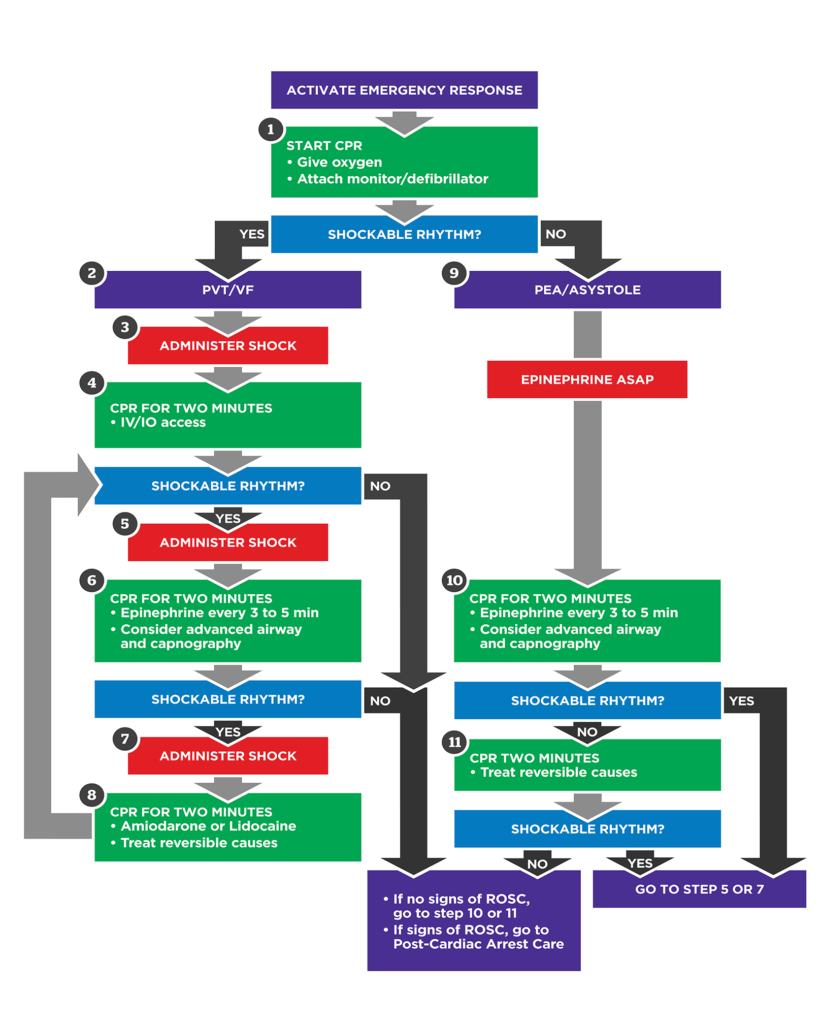
3. ACLS Cardiac Arrest Algorithms
A. Shockable Rhythm (VF / Pulseless VT)
- Start CPR → Attach defibrillator
- Shock #1
- CPR 2 min → IV/IO access
- Shock #2
- CPR + Epinephrine 1 mg IV/IO every 3–5 min
- Shock #3
- CPR + Amiodarone 300 mg IV bolus
* Second dose: 150 mg
- Continue cycles + treat Hs and Ts
B. Non-Shockable Rhythm (Asystole / PEA)
- CPR immediately
- IV/IO access
- Epinephrine 1 mg IV/IO every 3–5 min
- Reassess rhythm every 2 min
- Identify and treat reversible causes
- Defibrillation is NOT indicated
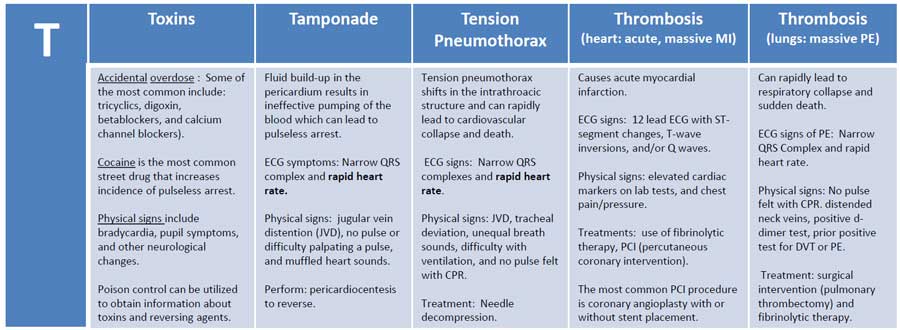
4. Reversible Causes – Hs and Ts
Hs
- Hypoxia
- Hypovolemia
- Hydrogen ion (acidosis)
- Hypo-/Hyperkalemia
- Hypothermia
Ts
- Tension pneumothorax
- Tamponade (cardiac)
- Toxins
- Thrombosis (coronary)
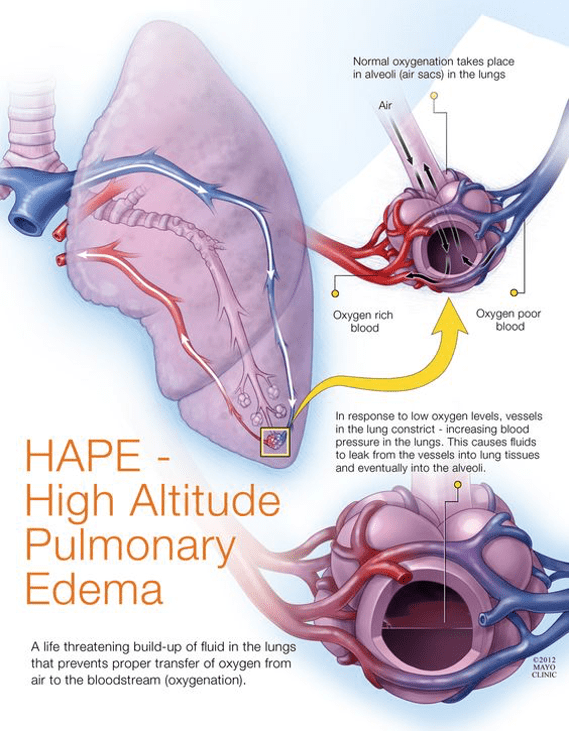
- Thrombosis (pulmonary)
5. Peri-Arrest Arrhythmia Management
A. Bradycardia (HR <50/min with symptoms)
Symptoms: hypotension, altered mental status, ischemia, shock
Management
- Atropine 1 mg IV every 3–5 min (max 3 mg)
- If ineffective:
* Transcutaneous pacing
* Dopamine infusion 5–20 mcg/kg/min
* Epinephrine infusion 2–10 mcg/min
B. Tachycardia (HR >150/min with pulse)
Step 1: Is the patient unstable?
- Hypotension
- Shock
- Chest pain
- Acute heart failure
- Altered mental status
➡ Immediate synchronized cardioversion
Step 2: Stable Tachycardia
##### Narrow QRS (<120 ms)
- Regular: Adenosine 6 mg IV rapid push → 12 mg if needed
- Irregular: Rate control (beta-blocker or calcium channel blocker)
##### Wide QRS (≥120 ms)
- Monomorphic VT: Amiodarone 150 mg IV over 10 min
- Polymorphic VT: Treat as VF (defibrillate)
6. ACLS Medications – Complete Drug Table
Epinephrine
- Indication: Cardiac arrest, bradycardia infusion
- Dose (arrest): 1 mg IV/IO every 3–5 min
- MOA: α-vasoconstriction, β-inotropy
- Adverse effects: Tachyarrhythmias, hypertension
Amiodarone
- Indication: Refractory VF/pVT, VT with pulse
- Dose (arrest): 300 mg IV bolus → 150 mg
- MOA: Class III antiarrhythmic
- Adverse effects: Hypotension, bradycardia
Lidocaine (alternative)
- Dose: 1–1.5 mg/kg IV bolus
- Use: If amiodarone unavailable
Atropine
- Indication: Symptomatic bradycardia
- Dose: 1 mg IV every 3–5 min (max 3 mg)
- MOA: Anticholinergic → ↑ SA/AV node firing
Adenosine
- Indication: Stable regular narrow-complex tachycardia
- Dose: 6 mg IV rapid push → 12 mg
- Contraindications: Asthma, irregular wide QRS
Magnesium Sulfate
- Indication: Torsades de Pointes
- Dose: 1–2 g IV over 5–20 min
7. Post–Cardiac Arrest Care
- Maintain SpO₂ 94–99%
- Avoid hypotension (MAP ≥65 mmHg)
- Targeted Temperature Management (TTM):
* 32–36°C for 24 hours (if comatose)
- Immediate 12-lead ECG
- Coronary angiography if STEMI or suspected ischemia
- Seizure control, glucose management
8. Termination of Resuscitation (TOR)
Consider when:
- Persistent asystole despite optimal ACLS
- No reversible causes
- End-tidal CO₂ persistently <10 mmHg after 20 min
- Medical futility and protocol compliance
9. ACLS Team Roles
- Team leader
- Compressor
- Airway manager
- Monitor/defibrillator operator
- IV/IO medication nurse
- Recorder/timekeeper
Effective ACLS requires closed-loop communication and role clarity.
10. Key ACLS Exam Pearls
- Shock VF/pVT, not asystole/PEA
- CPR quality > drugs
- Epinephrine for all cardiac arrest rhythms
- Amiodarone only after defibrillation
- Treat cause, not just rhythm