Diseases of the pericardium — complete clinical reference
Topics covered: Acute pericarditis, Pericardial effusion, Cardiac tamponade, Constrictive pericarditis.
No images. External links included.
Quick note: this is a comprehensive clinical summary for medical practitioners. It is educational and not a substitute for clinical judgement or local guidelines. When in doubt, consult your institution’s cardiology team and up-to-date guidelines.
1) Acute pericarditis
Definition
Acute pericarditis = inflammation of the pericardial layers (visceral + parietal) usually presenting with pleuritic chest pain, pericardial friction rub, ECG changes, ± pericardial effusion. Typical episode = ≤4–6 weeks. ([OUP Academic][1])
Pathophysiology
Inflammation (infectious—viral common; or noninfectious: autoimmune, uremic, post-MI, radiation, neoplastic) → pericardial inflammation, increased vascular permeability → exudation of fluid and inflammatory cells; biochemical mediators produce pain and ECG changes. Persistent inflammation can lead to recurrent pericarditis or to scarring → constrictive physiology. ([PMC][2])
Causes / triggers (common)
- Viral (coxsackie, echovirus, influenza, adenovirus, COVID-19 and others) — most common idiopathic presumed viral.
- Post-myocardial infarction (Dressler’s is autoimmune, later onset).
- Uremia (severe renal failure).
- Autoimmune/connective tissue disease (SLE, RA).
- Neoplastic infiltration (metastasis).
- Radiation, trauma, post-cardiac surgery.
- Bacterial/tuberculous pericarditis (important in high-TB prevalence areas). ([PMC][2])
Clinical features
- Chest pain: sharp, pleuritic, improves leaning forward, worse on inspiration/supine.
- Fever (variable).
- Pericardial friction rub (highly specific but transient).
- Dyspnea if effusion.
- Signs of systemic illness if infectious/malignant.
- ECG: Stage I diffuse ST-segment elevation with PR depression (leads with epicardial injury pattern), later T wave changes. ([OUP Academic][1])
Investigations / diagnosis
Diagnostic criteria (any two of four): typical chest pain, pericardial friction rub, ECG changes characteristic of pericarditis, new pericardial effusion. Support with elevated CRP/ESR. - Echocardiography to detect effusion and hemodynamic effect. Chest X-ray and CT/CMR when needed (CMR detects pericardial inflammation/fibrin). Consider blood cultures if febrile or suspect bacterial. Pericardiocentesis and fluid analysis only when diagnostic uncertainty, large effusion, tamponade or suspected bacterial/malignant/TB cause. ([OUP Academic][1])
Differential diagnoses
- Acute myocardial ischemia / STEMI (distinguish by focal ST changes, biomarkers and history).
- Pulmonary embolism, aortic dissection, pleuritis, musculoskeletal chest pain, esophageal disease. ([OUP Academic][1])
Management — stepwise (medical practitioner)
General principles: treat inflammation and the underlying cause; relieve pain; monitor for effusion/tamponade; avoid unnecessary invasive procedures.
- Initial triage
* Evaluate stability, vitals, signs of tamponade. Urgent echo if effusion suspected or unstable. ([Heart University][3])
- First-line anti-inflammatory therapy (unless contraindicated)
* NSAIDs: e.g., ibuprofen or aspirin (high anti-inflammatory doses) + colchicine for 3 months (first episode) or 6 months (recurrent) — colchicine reduces recurrence. Avoid NSAIDs if suspected myocardial injury where aspirin preferred (post-MI dosing differs). ([European Society of Cardiology][4])
- Colchicine: added to NSAID regimen for most patients (improves recovery, reduces recurrence). Dose adjustments for renal function. ([European Society of Cardiology][4])
- Corticosteroids: use only if NSAIDs/colchicine contraindicated or in specific causes (autoimmune, uremic not responsive, inflammatory disease)—steroids increase recurrence risk if used inappropriately and should be low dose and tapered. ([OUP Academic][1])
- Pericardiocentesis: indicated if hemodynamic compromise/tamponade, purulent pericarditis, or for diagnostic sampling when cause unknown and will change management. Avoid routine aspiration for small effusions. ([European Society of Cardiology][5])
- Specific therapy: treat underlying cause — e.g., antitubercular therapy for tuberculous pericarditis; chemotherapy for malignant effusions when appropriate; dialysis for uremic pericarditis. ([PMC][2])
Non-pharmacologic measures
- Rest during acute severe pain; avoid strenuous activity until inflammation resolved and CRP normal.
- Monitor with serial echocardiography if effusion present. ([Heart University][3])
2) Pericardial effusion
Definition
Pericardial effusion = abnormal accumulation of fluid in pericardial space. Size and rate of accumulation determine clinical impact. ([PMC][2])
Pathophysiology
Same causes as pericarditis or secondary (malignancy, hypothyroidism, trauma). Rapid accumulation causes high intrapericardial pressure → compromised filling (tamponade) even with smaller volumes. Slow accumulation may allow large volumes with little hemodynamic effect. ([PMC][2])
Clinical features
- Often dyspnea, chest discomfort, cough, fatigue.
- Muffled heart sounds, enlarged cardiac silhouette on CXR if large, electrical alternans on ECG (large effusion). If tamponade develops: hypotension, tachycardia, JVP elevation. ([PMC][2])
Investigations
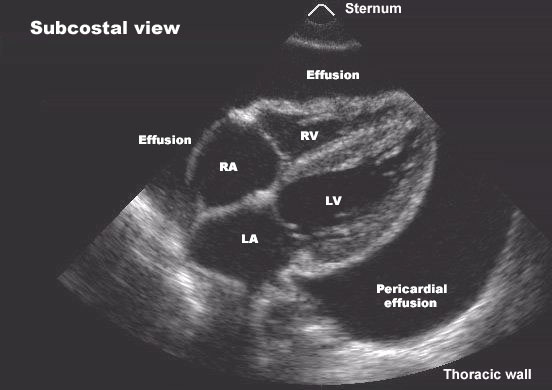
- Echocardiography (TTE) — first-line: quantifies effusion, detects RV diastolic collapse, IVC plethora (tamponade features).
- ECG (low voltage, electrical alternans), CXR (cardiomegaly if large), CT/CMR when further info needed; pericardial fluid analysis if pericardiocentesis done (cell count, Gram stain, culture, cytology, TB testing). ([ASE][6])
Management
- Small, asymptomatic effusion: observe, treat underlying cause, serial echo.
- Large effusion without tamponade: consider pericardiocentesis if symptomatic or uncertain cause; otherwise monitor.
- Pericardial tamponade / hemodynamic compromise: urgent pericardiocentesis (echo-guided) — definitive therapy. Pericardial window or surgical drainage if recurrent loculated effusions or malignant/purulent effusions. ([Medscape][7])
3) Cardiac tamponade (acute)
Definition
Life-threatening compression of heart due to pericardial fluid under pressure that impairs diastolic filling → reduced stroke volume and shock. ([NCBI][8])
Pathophysiology
Rise in intrapericardial pressure exceeds chamber filling pressures (especially right-sided) → impaired ventricular filling, decreased cardiac output. Rate of fluid accumulation is the critical determinant. ([NCBI][8])
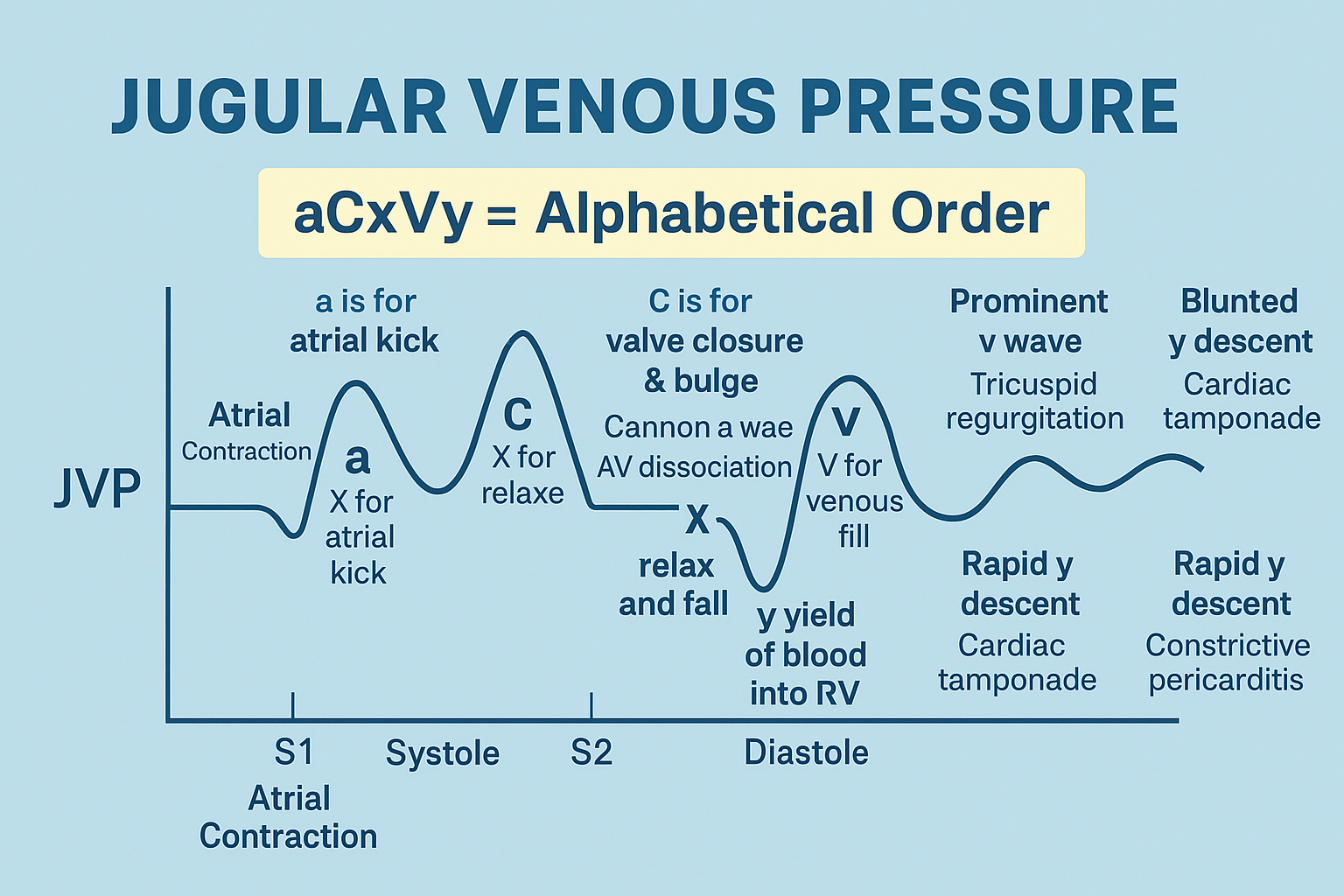
Clinical features (Beck’s triad classic but variable)
- Hypotension / shock;
- Elevated jugular venous pressure;
- Muffled heart sounds.
Other signs: tachycardia, pulsus paradoxus (>10 mmHg drop in systolic BP during inspiration), dyspnea, cool extremities. ([NCBI][8])
Investigations (urgent)
- Bedside TTE: look for RV diastolic collapse, right atrial collapse, respiratory variation of ventricular filling, IVC dilation without collapse — confirms tamponade physiology.
- ECG, pulse/BP monitoring, but do NOT delay drainage if high suspicion and instability. ([ASE][6])
Emergency management — stepwise
- Resuscitative measures while arranging definitive therapy: oxygen, large-bore IV access, crystalloid bolus (temporary increase in venous return), inotropes if needed (e.g., dobutamine) — these are temporizing. Avoid positive pressure ventilation if possible (worsens hemodynamics). ([European Society of Cardiology][9])
- Urgent pericardiocentesis (echo-guided) — immediate decompression is definitive. Pericardiocentesis should be done by experienced operator with appropriate monitoring; surgical drainage if loculated purulent effusion or when pericardiocentesis not feasible. ([Medscape][7])
- Post-drainage: monitor for re-accumulation; send fluid for analysis (cytology, cultures, TB tests) as indicated. Treat underlying cause. ([AHA Journals][10])
4) Constrictive pericarditis (chronic)
Definition
Pericardial scarring, fibrosis and/or calcification causing fixed, rigid pericardium that restricts diastolic filling → right-sided venous congestion and heart failure with preserved LV systolic function (often). May be transient (inflammatory) or chronic. ([PubMed][11])
Pathophysiology
Pericardial inelasticity → equalization of diastolic pressures, ventricular interdependence, impaired ventricular filling, elevated systemic venous pressures. Common final pathway of recurrent inflammation, radiation, cardiac surgery, TB. ([PubMed][11])
Causes / epidemiology
- Developed world: idiopathic/viral, postsurgical, radiation.
- Developing world / high TB prevalence: tuberculous pericarditis is important cause. ([European Society of Cardiology][12])
Clinical features
- Progressive exertional dyspnea, fatigue; signs of right heart failure: jugular venous distension, Kussmaul sign (JVP fails to fall on inspiration), peripheral edema, ascites, hepatic congestion; pericardial knock (early diastolic sound). ([PubMed][11])
Investigations
- ECG: low voltage, nonspecific;
- CXR: pericardial calcification (not always present);
- Echocardiography: abnormal ventricular filling, septal bounce, respiratory variation;
- CT/CMR: pericardial thickening, calcification, myocardial tagging; CMR shows pericardial inflammation (may be reversible).
- Cardiac catheterization (invasive): shows equalization of diastolic pressures and dip-and-plateau appearance — useful when diagnosis uncertain. ([LWW Journals][13])
Management
- Identify reversible (inflammatory) constriction: if active inflammation (elevated CRP, CMR evidence) → trial of anti-inflammatory therapy (NSAIDs ± colchicine ± steroids) and close follow-up; some cases may recover and avoid surgery. ([LWW Journals][13])
- Definitive therapy for chronic constriction: pericardiectomy (surgical removal of pericardium) — indicated for persistent symptomatic constriction; timing individualized. Pericardiectomy carries operative risk (higher if prior radiation, advanced disease). ([PubMed][11])
- Medical management: diuretics to control congestion; treat underlying cause (anti-TB therapy when tuberculous), optimize comorbidities. Diuretics relieve symptoms but do not reverse constriction. ([PubMed][11])
5) Drugs mentioned — required practical details
> For each drug below: indication (in pericardial disease), mechanism, usual dosing (adult and paediatric if relevant), short PK summary, important adverse effects, contraindications, major drug–drug interactions, monitoring, patient counselling.
Ibuprofen (NSAID)
- Indication: first-line anti-inflammatory for acute pericarditis (when not post-MI).
- Mechanism: nonselective COX-1/COX-2 inhibitor → reduced prostaglandin synthesis → anti-inflammatory and analgesic.
- Usual dosing (adult): 600–800 mg orally every 6–8 hours (total 1.8–2.4 g/day) until symptom resolution and CRP normalizes; then taper. Pediatric: dosing weight-based (e.g., 30–40 mg/kg/day divided q6–8h) — check local paediatric protocol. Adjust for renal disease. ([European Society of Cardiology][4])
- PK (brief): oral bioavailability good, peak 1–2 h, hepatic metabolism, renal excretion of metabolites.
- Common/serious AEs: GI irritation/bleed, renal impairment, increased cardiovascular risk at high chronic doses, hypersensitivity.
- Contraindications: active peptic ulcer/GI bleed, severe renal impairment, NSAID hypersensitivity, third trimester pregnancy (risk to ductus).
- Interactions: anticoagulants (↑bleeding), ACE inhibitors/ARBs (↓renal function), diuretics (risk renal).
- Monitoring: symptom relief, BP, renal function, signs of GI bleeding, CRP for disease activity.
- Counsel: take with food, avoid NSAIDs if aspirin used for post-MI indications without cardiology advice.
Aspirin
- Indication: preferred in pericarditis post-MI (Dressler’s) and when NSAIDs contraindicated in that context.
- Mechanism: irreversible COX inhibitor.
- Adult dosing (pericarditis post-MI): high dose (e.g., 650–1000 mg every 6–8 h) — follow cardiology/post-MI guidance. Pediatric: not used in viral illness (Reye’s risk).
- PK/AEs/Interactions/Monitoring/Counsel: similar to NSAIDs (GI bleeding, bleeding risk), check platelet/bleeding history.
Colchicine
- Indication: adjunct for acute and recurrent pericarditis (reduces recurrence and improves symptom resolution).
- Mechanism: inhibits microtubule polymerization, reduces neutrophil activity and inflammasome activation.
- Dosing (adult): 0.5–0.6 mg twice daily for >70 kg or 0.5 mg once daily if <70 kg — typical durations: 3 months (first episode) or 6 months (recurrent). Adjust for renal impairment. Pediatric: weight-based dosing; specialist guidance recommended. ([European Society of Cardiology][4])
- PK: oral, hepatic metabolism via CYP3A4 and P-glycoprotein; renal excretion of metabolites.
- AEs: GI upset (diarrhea, nausea), rare myopathy (esp. with statins), neutropenia, bone marrow suppression (rare).
- Contraindications: severe renal or hepatic impairment (dose adjust/avoid), concurrent strong CYP3A4 or P-gp inhibitors (e.g., clarithromycin, some antifungals) — increases toxicity risk.
- Monitoring: renal/hepatic function, muscle symptoms if on statins, CBC if prolonged use.
- Counsel: expect GI side effects; report muscle pain/weakness; avoid grapefruit and certain interacting drugs.
Corticosteroids (e.g., Prednisone)
- Indication: second-line for autoimmune or refractory pericarditis, or when NSAIDs/colchicine contraindicated. Avoid routine use for idiopathic viral pericarditis due to higher recurrence risk.
- Mechanism: broad anti-inflammatory and immunosuppressive.
- Dosing (adult): low dose (e.g., prednisone 0.2–0.5 mg/kg/day) with slow taper tailored to response; higher doses for autoimmune disease. Pediatric: specialist dosing. ([OUP Academic][1])
- AEs: hyperglycemia, immunosuppression, osteoporosis, weight gain, mood changes, adrenal suppression.
- Contraindications/interactions: active uncontrolled infection, live vaccines; interacts with many drugs (enzyme inducers/inhibitors).
- Monitoring: glucose, BP, signs infection, bone health if long-term.
- Counsel: taper gradually; avoid abrupt stop; report infection symptoms.
Diuretics (e.g., Furosemide)
- Indication: symptomatic relief of congestion in constrictive pericarditis and heart-failure symptoms. Not disease-modifying.
- Mechanism: loop diuretic → inhibit Na-K-2Cl transporter → diuresis.
- Dosing: individualized; monitor electrolytes.
- AEs: electrolyte disturbances, renal function changes.
- Monitoring: renal function, electrolytes, weight, blood pressure.
Inotropes (e.g., Dobutamine)
- Indication: temporary hemodynamic support in tamponade prior to drainage if needed.
- Mechanism: β-adrenergic agonist increasing cardiac contractility.
- Use: short-term IV infusion in ICU; not substitute for drainage.
Anti-tubercular therapy (ATT)
- Indication: tuberculous pericarditis (when diagnosed or highly suspected).
- Principle: full course ATT per national TB program; adjunctive steroids may be used in certain tuberculous pericarditis presentations to reduce constriction risk — follow national/international TB guidance. ([PubMed][11])
6) Procedural considerations
- Pericardiocentesis: image-guided (echo or CT), trained operator, sterile technique, drain placement if large/purulent/malignant, send fluid for cell count/Gram/culture/cytology/ADA/TB PCR as indicated. Risks: bleeding, laceration, arrhythmia, pneumothorax. ([European Society of Cardiology][5])
- Surgical pericardial window / pericardiectomy: indicated for recurrent malignant or loculated effusions, purulent pericarditis, or symptomatic chronic constriction (pericardiectomy definitive). Pericardiectomy is major surgery with significant perioperative risk in advanced disease. ([PubMed][11])
7) Prognosis & follow-up
- Prognosis depends on cause: idiopathic/viral cases often recover with treatment; malignant, purulent and tuberculous causes carry higher morbidity/mortality. Recurrent pericarditis risk reduced by colchicine. Constrictive pericarditis may require surgery; outcomes depend on etiology and comorbidity. Serial echo, CRP and clinical review guide follow-up. ([European Society of Cardiology][4])
8) Practical quick reference (when to drain)
- Urgent pericardiocentesis: signs of tamponade/hemodynamic compromise.
- Consider drainage: large symptomatic effusion, suspected purulent or malignant/TB cause for diagnosis/therapy.
- Observe/medical therapy: small effusion without tamponade and clear inflammatory pericarditis responding to NSAIDs/colchicine. ([Medscape][7])
9) Selected high-quality external references (read these for detailed protocols)
- 2015 ESC Guidelines — Diagnosis and management of pericardial diseases (Eur Heart J). ([OUP Academic][1])
- Recent review: Diagnosis, treatment, and management of pericardial diseases (NCBI/PMC). ([PMC][2])
- StatPearls: Cardiac Tamponade (NCBI Bookshelf / clinical overview). ([NCBI][8])
- ESC practical articles on pericardiocentesis and constrictive pericarditis reviews (E-J of Cardiology Practice / ESC pages). ([European Society of Cardiology][5])
- Multimodality imaging for pericardial disease (ASE/CMR/CT primer). ([ASE][6])
10) Key practical clinical pearls
- Any unstable patient with suspected tamponade → do not delay pericardial decompression for prolonged testing. Echo is quick and diagnostic if available. ([European Society of Cardiology][9])
- Always search for underlying cause — management differs (TB, malignancy, uremia).
- Colchicine is underused but strongly reduces recurrence; tailor dose to renal function and drug interactions. ([European Society of Cardiology][4])
- Steroids increase recurrence risk when used indiscriminately — restrict to specific indications. ([OUP Academic][1])