Pulseless Electrical Activity (PEA)
1. Definition
Pulseless Electrical Activity (PEA) is a cardiac arrest rhythm characterized by organized electrical activity on ECG without a palpable pulse or measurable cardiac output. Electrical depolarization occurs, but mechanical contraction is absent or ineffective, resulting in circulatory collapse.
> PEA is not a shockable rhythm.
2. Pathophysiology
PEA occurs when electromechanical dissociation develops due to:
- Severely reduced preload, afterload mismatch, myocardial pump failure, or obstructed cardiac filling/outflow
- Cellular hypoxia, acidosis, or metabolic derangements impairing excitation–contraction coupling
- Catastrophic mechanical causes (tamponade, massive PE, tension pneumothorax)
Electrical conduction persists, but stroke volume → zero.
3. Etiology (Reversible Causes – “Hs and Ts”)
Hs
- Hypovolemia – hemorrhage, dehydration
- Hypoxia – airway obstruction, respiratory failure
- Hydrogen ion (Acidosis) – lactic, renal failure
- Hypo-/Hyperkalemia – renal failure, drugs
- Hypothermia – exposure, cold environments
- Hypoglycemia (considered in some protocols)
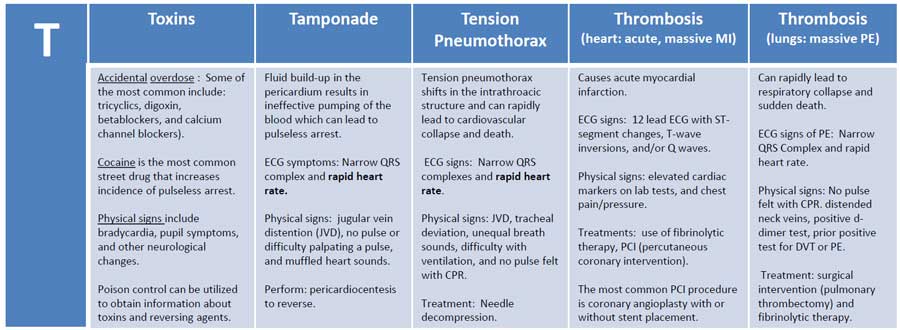
Ts
- Tension pneumothorax
- Cardiac tamponade
- Toxins – beta-blockers, calcium channel blockers, opioids, TCAs
- Thrombosis (coronary) – acute MI
- Thrombosis (pulmonary) – massive pulmonary embolism
- Trauma – severe blunt or penetrating injury
4. Clinical Features
- Unresponsiveness
- Absent carotid/femoral pulse
- Apnea or agonal respirations
- ECG shows organized rhythm (sinus, junctional, idioventricular)
- No blood pressure, no cardiac output
5. Diagnosis
PEA is a clinical diagnosis during cardiac arrest.
Key Diagnostic Points
- ECG rhythm without pulse
- Confirm with pulse check ≤10 seconds
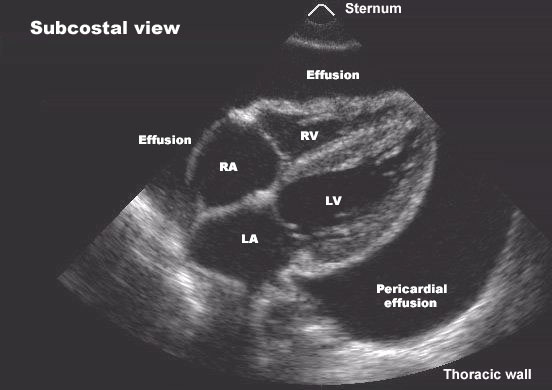
- Point-of-care ultrasound (POCUS) (highly valuable):
* Distinguish true PEA (no cardiac activity)
* Identify reversible causes (tamponade, massive PE, hypovolemia)
6. Differential Diagnosis
- Asystole (no electrical activity)
- Ventricular fibrillation
- Pulseless ventricular tachycardia
- Profound cardiogenic shock with weak pulse
- Pseudo-PEA (minimal cardiac output detectable only by ultrasound)
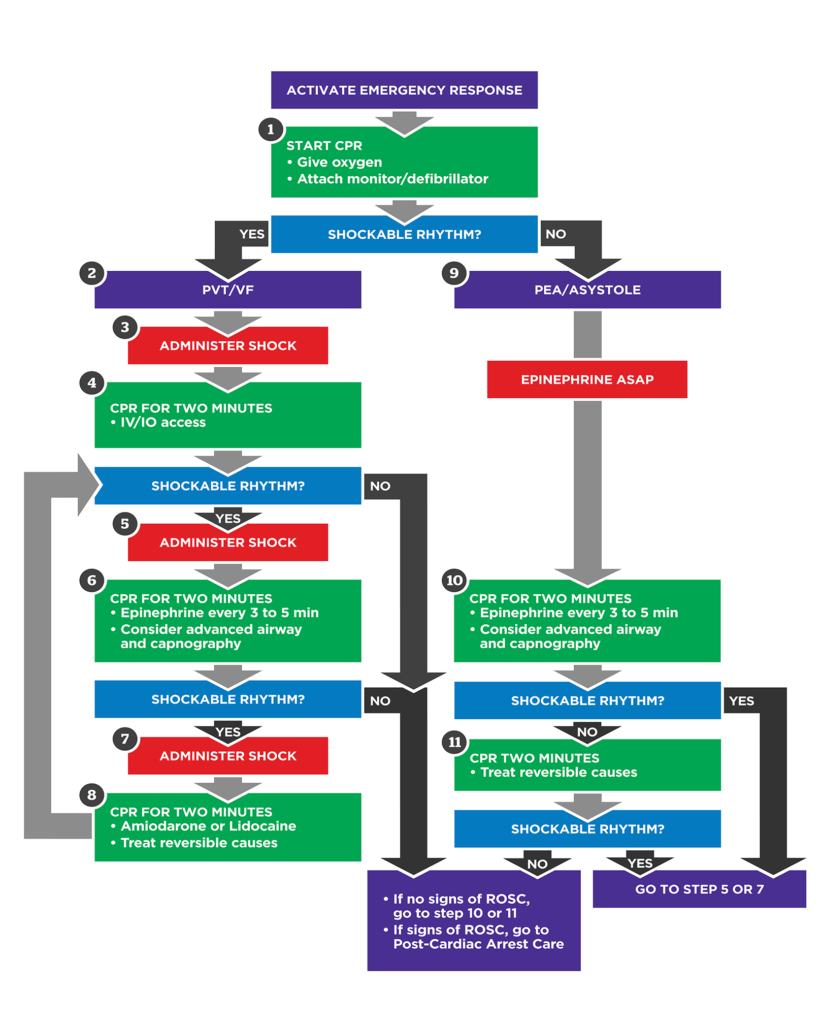
7. Management (ACLS – Stepwise)
Immediate Actions
- High-quality CPR
* Rate: 100–120/min
* Depth: 5–6 cm
* Full recoil, minimal interruptions
- Airway & Oxygen
* 100% oxygen
* Early advanced airway if skilled
- IV/IO Access
Drug Therapy
Epinephrine
- Indication: All PEA cardiac arrests
- Dose:
* Adults: 1 mg IV/IO every 3–5 minutes
* Pediatrics: 0.01 mg/kg IV/IO (1:10,000), max 1 mg
- Mechanism:
* α1: peripheral vasoconstriction → ↑ coronary & cerebral perfusion
* β1: ↑ myocardial contractility
- Pharmacokinetics: Rapid onset, short half-life (~2–3 min)
- Adverse Effects: Tachyarrhythmias, myocardial ischemia (post-ROSC)
- Contraindications: None in cardiac arrest
- Monitoring: Rhythm checks every 2 min, ETCO₂
- Counseling: Not applicable (emergency drug)
Critical Principle
👉 Identify and treat reversible causes (Hs & Ts)
Drugs alone will not reverse PEA without correcting the cause.
8. Cause-Specific Management
| Cause | Targeted Treatment |
| -------------------- | ------------------------------------------------------------- |
| Hypovolemia | Rapid IV crystalloids, blood products |
| Hypoxia | Secure airway, ventilate with 100% O₂ |
| Acidosis | Effective CPR, ventilation; sodium bicarbonate only if severe |
| Hyperkalemia | Calcium gluconate, insulin + glucose, beta-agonists |
| Tension pneumothorax | Immediate needle decompression |
| Cardiac tamponade | Emergency pericardiocentesis |
| Massive PE | Thrombolysis or embolectomy |
| Coronary thrombosis | Emergent PCI after ROSC |
| Toxins | Antidotes (naloxone, glucagon, calcium), supportive care |
| Hypothermia | Active rewarming |
9. Role of Ultrasound in PEA
- Confirms cardiac standstill vs pseudo-PEA
- Guides fluid resuscitation
- Detects tamponade, PE, pneumothorax
- Prognostic value (persistent standstill → poor prognosis)
10. Prognosis
- Overall survival is poor compared to shockable rhythms
- Better outcomes when:
* PEA is secondary to reversible causes
* Early CPR and early epinephrine
* POCUS-guided management
- Prolonged true PEA with no reversible cause → very high mortality
11. Post-ROSC Care
- Maintain SpO₂ 94–98%
- Avoid hypotension (MAP ≥65 mmHg)
- Targeted temperature management if comatose
- Treat underlying cause definitively
- Neurologic monitoring
12. Key Exam & Clinical Pearls
- PEA = electrical activity WITHOUT pulse
- Not shockable
- CPR + epinephrine + fix the cause
- Always think Hs and Ts
- Ultrasound is a game-changer