Definition
Bundle Branch Block (BBB) is an intraventricular conduction abnormality where electrical impulse transmission through the right or left bundle branch of the His–Purkinje system is delayed or blocked. This results in asynchronous ventricular depolarization and characteristic ECG changes.
Anatomy and Pathophysiology
- Normal conduction: SA node → AV node → His bundle → Right Bundle Branch (RBB) + Left Bundle Branch (LBB) → Purkinje fibers.
- In BBB:
* The blocked ventricle is activated indirectly via cell-to-cell conduction from the opposite ventricle.
* This causes QRS widening ≥ 120 ms.
* Mechanical dyssynchrony may impair cardiac output, especially in LBBB.
Types of Bundle Branch Block
1. Right Bundle Branch Block (RBBB)
- Delay in right ventricular depolarization
- Often benign if isolated
2. Left Bundle Branch Block (LBBB)
- Delay in left ventricular depolarization
- Strongly associated with structural heart disease
- Masks ischemic ECG changes
3. Incomplete BBB
- Same morphology as BBB
- QRS duration 110–119 ms
4. Bifascicular Block
- RBBB + Left Anterior Fascicular Block (LAFB)
- RBBB + Left Posterior Fascicular Block (LPFB)
5. Trifascicular Disease
- Bifascicular block + AV nodal delay (PR prolongation)
- High risk of complete heart block
Etiology
Common Causes
RBBB
- Normal variant (young, healthy individuals)
- Pulmonary embolism
- Chronic lung disease (cor pulmonale)
- Atrial septal defect
- Right ventricular strain
- Ischemic heart disease
LBBB
- Hypertension with LV hypertrophy
- Ischemic heart disease / MI
- Dilated or hypertrophic cardiomyopathy
- Aortic stenosis
- Degenerative conduction system disease (Lenègre/Lev disease)
Both
- Myocarditis
- Cardiac surgery
- Electrolyte abnormalities (hyperkalemia)
- Drugs: Class I antiarrhythmics
Clinical Features
Symptoms
- Often asymptomatic
- If present:
* Dizziness
* Syncope (suggests high-grade conduction disease)
* Dyspnea, fatigue (especially LBBB with heart failure)
* Palpitations
Signs
- Usually none
- In LBBB: paradoxical splitting of S2
- In advanced disease: bradycardia, hypotension
Electrocardiographic Diagnosis
General Criteria
- QRS duration ≥ 120 ms
- Broad, slurred QRS complexes
RBBB ECG Features
- QRS ≥ 120 ms
- rSR′ pattern in V1–V2 (“rabbit ears”)
- Broad terminal S wave in I, V5, V6
- Normal ST-T changes opposite QRS (secondary repolarization)
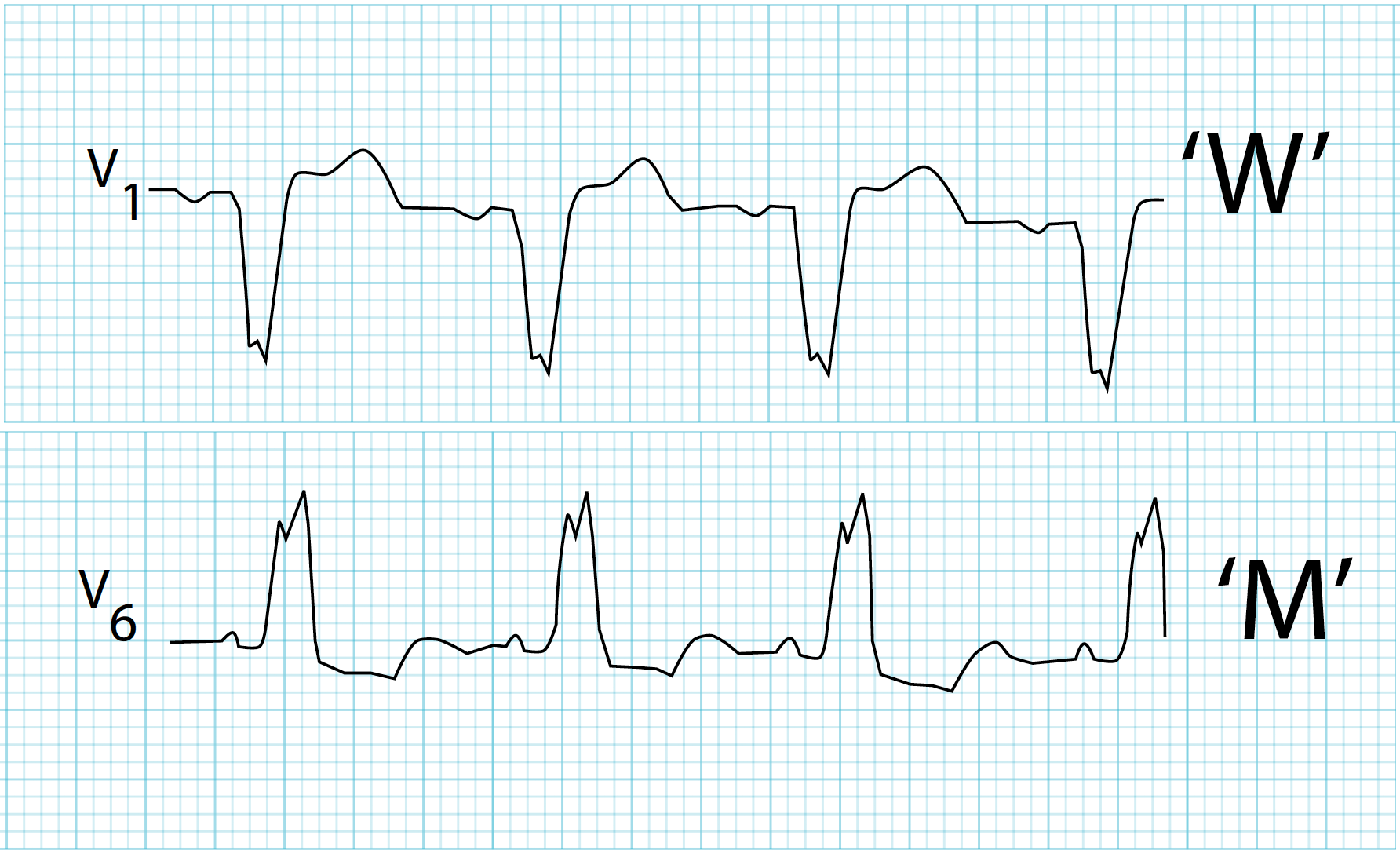
LBBB ECG Features
- QRS ≥ 120 ms
- Broad, notched (“M-shaped”) R wave in I, aVL, V5–V6
- Deep S waves in V1–V3
- Absence of Q waves in lateral leads
- ST-T discordance
- Ischemia detection difficult
Important Clinical Rules
- New-onset LBBB + chest pain = treat as STEMI equivalent
- RBBB does not obscure MI diagnosis
- LBBB suggests underlying heart disease until proven otherwise
Investigations
Baseline
- 12-lead ECG (diagnostic)
- Echocardiography
* LV function
* Structural heart disease
* Valvular pathology
Additional Tests
- Cardiac enzymes (if ACS suspected)
- Holter monitoring (syncope, intermittent block)
- Stress testing (modified protocols for LBBB)
- Coronary angiography (if ischemia suspected)
- Electrophysiology study (recurrent syncope, advanced block)
Differential Diagnosis
- Ventricular paced rhythm
- Ventricular tachycardia
- Hyperkalemia
- Pre-excitation (WPW)
- Nonspecific intraventricular conduction delay
Management
Asymptomatic Isolated BBB
- No specific treatment
- Periodic follow-up
- Treat underlying condition if present
Symptomatic BBB
Management depends on cause and severity:
Underlying Disease Treatment
- Ischemic heart disease → Revascularization
- Heart failure → Guideline-directed medical therapy
- Hypertension → Optimal BP control
- Valvular disease → Surgical/interventional correction
Pacemaker Indications
- BBB with:
* Syncope due to high-grade AV block
* Alternating bundle branch block
* Trifascicular disease with symptoms
* Advanced second- or third-degree AV block
Cardiac Resynchronization Therapy (CRT)
Indicated in LBBB with:
- Heart failure (NYHA II–IV)
- LVEF ≤ 35%
- QRS ≥ 150 ms
- Sinus rhythm
CRT improves:
- Symptoms
- LV function
- Survival
Prognosis
RBBB
- Excellent if isolated
- Prognosis depends on underlying cause
LBBB
- Worse prognosis
- Increased risk of:
* Heart failure
* Sudden cardiac death
* Cardiovascular mortality
Special Clinical Scenarios
BBB in Acute Myocardial Infarction
- New LBBB → emergency reperfusion
- RBBB + anterior MI → poor prognosis
BBB in Athletes
- Incomplete RBBB common and benign
- LBBB always pathological
BBB in Elderly
- Often degenerative
- Monitor for progression to complete heart block
Key Take-Home Points
- BBB = intraventricular conduction delay with wide QRS
- RBBB may be benign; LBBB is always significant
- New LBBB with chest pain = treat as MI
- CRT is life-saving in selected LBBB heart failure patients
- Management focuses on cause, symptoms, and conduction risk