Hyperthyroidism – Complete Clinical Reference
Definition
Hyperthyroidism is a clinical syndrome caused by excessive synthesis and/or release of thyroid hormones (T3 and T4) from the thyroid gland, leading to a hypermetabolic state affecting nearly all organ systems.
> Note: Thyrotoxicosis refers to excess circulating thyroid hormones from any cause, while hyperthyroidism specifically implies overproduction by the thyroid gland.
Epidemiology
- Prevalence: ~1–2% of population
- Female : Male = 5–10 : 1
- Peak age: 20–50 years
- Most common cause worldwide: Graves’ disease
- In iodine-deficient areas: toxic multinodular goiter
Physiology of Thyroid Hormones (Brief)
- T4 (thyroxine) → converted peripherally to T3 (triiodothyronine)
- T3 increases:
* Basal metabolic rate
* β-adrenergic receptor sensitivity
* Oxygen consumption
* Heat production
- Regulated by hypothalamic–pituitary–thyroid axis (TRH → TSH → T3/T4)
Pathophysiology
Excess thyroid hormones cause:
- ↑ Na⁺/K⁺-ATPase activity → ↑ energy expenditure
- ↑ β-adrenergic activity → tachycardia, tremors
- ↑ bone turnover → osteoporosis
- ↑ hepatic gluconeogenesis → glucose intolerance
- ↑ GI motility → diarrhea
- ↑ CNS excitability → anxiety, insomnia
Etiology / Causes
A. Primary Hyperthyroidism (TSH-independent)
- Graves’ disease (most common)
* Autoimmune (TSH-receptor stimulating antibodies)
- Toxic multinodular goiter
- Toxic adenoma
- Thyroiditis
* Subacute (De Quervain)
* Painless / postpartum
- Iodine-induced hyperthyroidism
- Drug-induced
* Amiodarone (Type I)
- Factitious thyrotoxicosis (exogenous hormone)
B. Secondary Hyperthyroidism (TSH-dependent)
- TSH-secreting pituitary adenoma (rare)
Clinical Features
General
- Weight loss despite ↑ appetite
- Heat intolerance
- Excessive sweating
- Fatigue, muscle weakness (proximal myopathy)
Cardiovascular
- Palpitations
- Tachycardia
- Atrial fibrillation
- Widened pulse pressure
- High-output heart failure (elderly)
Neurological / Psychiatric
- Anxiety, irritability
- Tremors
- Insomnia
- Emotional lability
- Hyperreflexia
Gastrointestinal
- Diarrhea
- Increased bowel frequency
- Abdominal discomfort
Dermatological
- Warm, moist skin
- Fine hair, hair loss
- Onycholysis (Plummer nails)
Musculoskeletal
- Proximal muscle wasting
- Osteopenia / osteoporosis
Reproductive
- Oligomenorrhea / amenorrhea
- Infertility
- Gynecomastia (men)
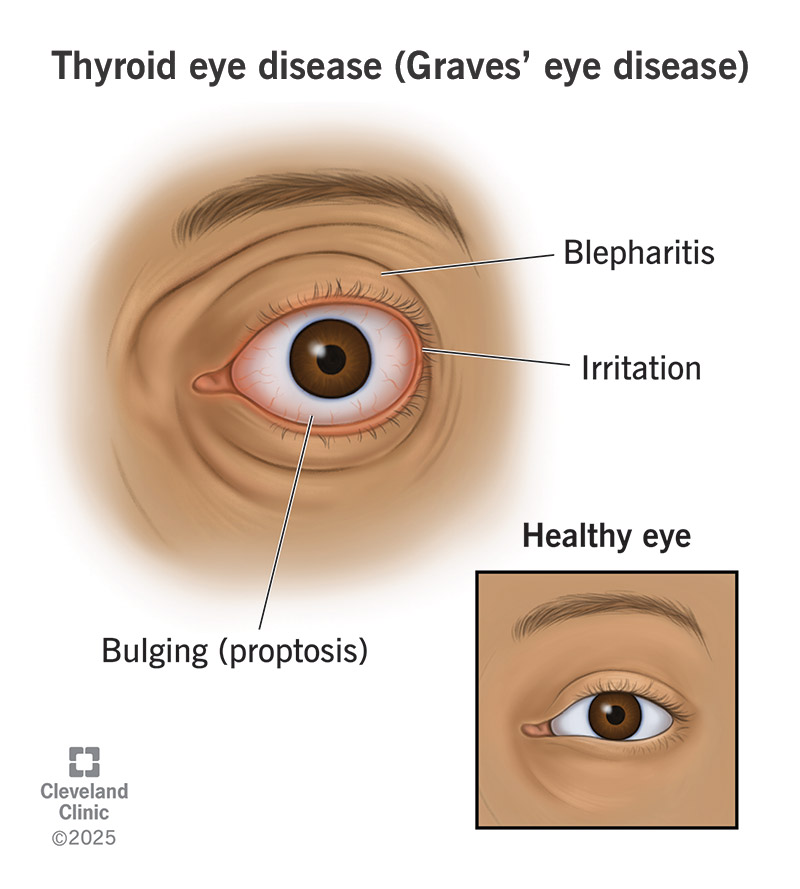
Eye Signs (Graves’ disease)
- Lid lag
- Proptosis
- Diplopia
- Exposure keratitis
Thyroid Storm (Medical Emergency)
Severe, life-threatening thyrotoxicosis
Features
- Hyperpyrexia
- Severe tachycardia
- Delirium / coma
- Heart failure
Investigations / Diagnosis
Thyroid Function Tests
| Test | Finding |
| ------- | ------------------------- |
| TSH | ↓↓↓ (suppressed) |
| Free T4 | ↑ |
| Free T3 | ↑ (T3-toxicosis possible) |
Autoantibodies
- TSH-receptor antibody (TRAb): positive in Graves’
- Anti-TPO: often positive
Imaging
- Radioactive iodine uptake (RAIU)
* High diffuse uptake → Graves’
* Focal uptake → Toxic adenoma
* Low uptake → Thyroiditis
- Thyroid ultrasound with Doppler
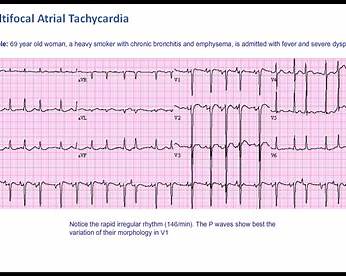
ECG
- Atrial fibrillation
- Sinus tachycardia
Others
- ↑ ALP (bone turnover)
- Mild hypercalcemia
- Low cholesterol
Differential Diagnosis
- Anxiety disorder
- Pheochromocytoma
- Subacute thyroiditis
- Factitious thyrotoxicosis
- Menopause
- Malignancy-associated weight loss
Management (Stepwise)
1. Symptomatic Treatment
Beta-Blockers
Indication: Control adrenergic symptoms
- Propranolol
* Mechanism: β-blockade + inhibits peripheral T4 → T3 conversion
* Dose: 20–40 mg orally every 6–8 hours
* Adverse effects: Bradycardia, bronchospasm
* Contraindications: Asthma, heart block
* Monitoring: Heart rate, BP
* Counselling: Do not stop abruptly
2. Antithyroid Drugs (ATDs)
Methimazole (Carbimazole → Methimazole)
- Indication: First-line in most patients
- Mechanism: Inhibits thyroid peroxidase → ↓ hormone synthesis
- Dose:
* Mild: 10–20 mg/day
* Severe: 30–40 mg/day
- Adverse effects:
* Rash
* Agranulocytosis (rare but serious)
* Hepatotoxicity (cholestatic)
- Contraindications: First trimester pregnancy (relative)
- Monitoring: CBC, LFTs
- Counselling: Report fever or sore throat immediately
Propylthiouracil (PTU)
- Indication: First trimester pregnancy, thyroid storm
- Mechanism: Inhibits TPO + T4 → T3 conversion
- Dose: 100–150 mg every 8 hours
- Adverse effects: Severe hepatotoxicity
- Monitoring: LFTs
- Counselling: Avoid alcohol
3. Radioactive Iodine Therapy (I-131)
- Indication: Graves’, toxic nodular goiter
- Mechanism: Destroys thyroid tissue
- Contraindications: Pregnancy, breastfeeding
- Complication: Permanent hypothyroidism
- Counselling: Radiation precautions
4. Surgery (Thyroidectomy)
- Indications:
* Large goiter
* Compression symptoms
* Malignancy suspicion
* ATD intolerance
- Complications:
* Hypocalcemia
* Recurrent laryngeal nerve injury
* Hypothyroidism
Management of Thyroid Storm
- PTU (loading dose)
- Propranolol
- Iodine (Lugol’s iodine) – after ATD
- Glucocorticoids
- Supportive care (fluids, cooling)
Special Situations
Pregnancy
- 1st trimester: PTU
- 2nd–3rd trimester: Methimazole
- Avoid radioactive iodine
Elderly
- Often present with apathetic hyperthyroidism
- High risk of atrial fibrillation
Prognosis
- Graves’: remission in ~40–50% with ATDs
- Radioiodine → lifelong hypothyroidism common
- Early diagnosis improves cardiovascular outcomes
Key Exam & Clinical Pearls
- Suppressed TSH = hallmark
- Graves’ = only cause with ophthalmopathy
- PTU preferred in thyroid storm
- Always check CBC before ATDs
- Beta-blockers relieve symptoms, not hormone excess