CASE 1: Dorsal Column Lesion (Proprioceptive Loss)
Scenario:
A 45-year-old man complains of difficulty walking in the dark. He cannot feel vibration over the medial malleolus, and joint position sense is lost in both lower limbs. Pain and temperature are normal.
Explanation:
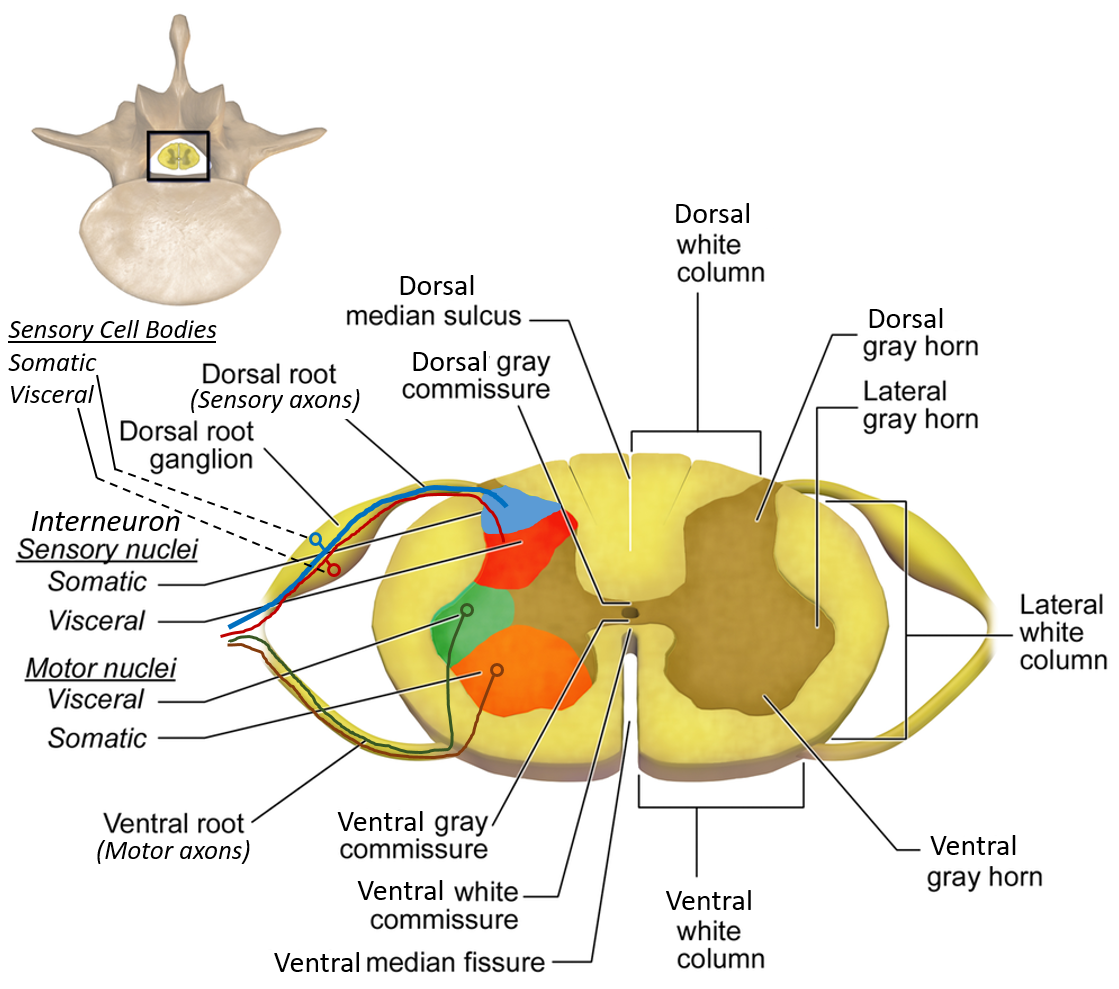
The dorsal columns (fasciculus gracilis) carry vibration and conscious proprioception from the lower limbs. These fibers ascend ipsilaterally.
Diagnosis:
Dorsal column dysfunction (e.g., vitamin B12 deficiency).
Management:
Check serum B12, start parenteral vitamin B12, physiotherapy for gait training.
CASE 2: Spinothalamic Tract Lesion
Scenario:
A 32-year-old woman presents with loss of pain and temperature sensation on the left side of the body below the level of T8, while touch and proprioception are intact.
Explanation:
Spinothalamic fibers cross within 1–2 spinal segments, so a right-sided lesion causes contralateral loss of pain and temperature.
Diagnosis:
Right spinothalamic tract lesion.
Management:
MRI spine to identify compression or tumor, analgesics, treat underlying cause.
CASE 3: Brown-Sequard Syndrome
Scenario:
After a stab injury to the right side of the spine at T10, a patient develops right-sided paralysis and loss of vibration sense, with loss of pain and temperature on the left side.
Explanation:
Hemisection damages:
- Ipsilateral corticospinal and dorsal column
- Contralateral spinothalamic tract
Diagnosis:
Brown-Sequard syndrome.
Management:
Spinal stabilization, corticosteroids if indicated, surgical repair, rehabilitation.
CASE 4: Anterior Spinal Artery Syndrome
Scenario:
A patient with severe hypotension suddenly develops paraplegia. Pain and temperature are lost, but vibration and proprioception are preserved.
Explanation:
Anterior spinal artery supplies anterior two-thirds of spinal cord (motor + spinothalamic). Dorsal columns are spared.
Diagnosis:
Anterior spinal artery infarction.
Management:
Supportive care, maintain blood pressure, physiotherapy.
CASE 5: Syringomyelia
Scenario:
A young adult presents with painless burns on both hands. Examination shows loss of pain and temperature over shoulders and arms in a “cape-like” distribution.
Explanation:
A central cavitation damages crossing spinothalamic fibers at the anterior white commissure.
Diagnosis:
Syringomyelia.
Management:
MRI cervical spine, surgical decompression if progressive.
CASE 6: LMN Lesion (Anterior Horn Cell)
Scenario:
A patient develops flaccid paralysis of hand muscles with muscle wasting and fasciculations. Reflexes are absent.
Explanation:
Anterior horn contains lower motor neurons. Damage causes LMN signs.
Diagnosis:
Anterior horn cell disease (e.g., poliomyelitis).
Management:
Supportive care, physiotherapy, prevent deformities.
CASE 7: UMN Lesion
Scenario:
A stroke patient develops spastic paralysis of both lower limbs with exaggerated reflexes and positive Babinski sign.
Explanation:
Damage to corticospinal tract leads to loss of inhibitory control.
Diagnosis:
Upper motor neuron lesion.
Management:
Antispastic drugs (baclofen), physiotherapy, treat cause.
CASE 8: Conus Medullaris Syndrome
Scenario:
A patient presents with sudden bladder and bowel dysfunction, saddle anesthesia, and mild bilateral leg weakness.
Explanation:
Conus medullaris involves S2–S4 segments affecting sphincters.
Diagnosis:
Conus medullaris lesion.
Management:
Emergency MRI, surgical decompression.
CASE 9: Cauda Equina Syndrome
Scenario:
A man with lumbar disc herniation presents with severe radicular pain, asymmetric leg weakness, and urinary retention.
Explanation:
Compression of nerve roots below L1 produces LMN signs.
Diagnosis:
Cauda equina syndrome.
Management:
Emergency surgical decompression.
CASE 10: Spinocerebellar Tract Lesion
Scenario:
A patient walks with a broad-based gait but has normal muscle strength and normal pain sensation.
Explanation:
Spinocerebellar tracts carry unconscious proprioception for coordination.
Diagnosis:
Spinocerebellar tract dysfunction.
Management:
Physiotherapy, treat underlying etiology.
CASE 11: Clarke’s Column Lesion
Scenario:
A patient shows ipsilateral limb ataxia without loss of conscious sensation.
Explanation:
Clarke’s column gives rise to posterior spinocerebellar tract.
Diagnosis:
Lesion of Clarke’s nucleus.
Management:
Supportive rehabilitation.
CASE 12: Dorsal Root Ganglion Lesion
Scenario:
A patient with herpes zoster has severe dermatomal pain followed by sensory loss.
Explanation:
DRG contains cell bodies of sensory neurons.
Diagnosis:
DRG involvement (post-herpetic neuralgia).
Management:
Antivirals, neuropathic pain medications.
CASE 13: Lateral Horn Lesion
Scenario:
A patient with spinal trauma at T1 develops ipsilateral ptosis and miosis.
Explanation:
Interruption of sympathetic neurons causes Horner syndrome.
Diagnosis:
Lateral horn (sympathetic) lesion.
Management:
Treat underlying spinal injury.
CASE 14: Posterior Column Degeneration
Scenario:
A malnourished patient shows sensory ataxia and positive Romberg sign.
Explanation:
Posterior columns degenerate in B12 deficiency.
Diagnosis:
Subacute combined degeneration.
Management:
Vitamin B12 replacement.
CASE 15: Central Cord Syndrome
Scenario:
After a fall, an elderly patient has greater weakness in upper limbs than lower limbs.
Explanation:
Central cervical cord affects medial corticospinal fibers (upper limb).
Diagnosis:
Central cord syndrome.
Management:
Immobilization, steroids, rehabilitation.
CASE 16: Posterior Horn Lesion
Scenario:
Segmental loss of pain sensation at one spinal level.
Explanation:
Posterior horn processes incoming sensory input.
Diagnosis:
Posterior horn lesion.
Management:
Treat local pathology.
CASE 17: Fasciculus Gracilis Lesion
Scenario:
Loss of vibration and position sense in lower limbs only.
Explanation:
Fasciculus gracilis carries lower limb proprioception.
Diagnosis:
Selective gracile tract lesion.
Management:
Cause-specific treatment.
CASE 18: Fasciculus Cuneatus Lesion
Scenario:
A patient cannot recognize objects placed in the hand (astereognosis).
Explanation:
Cuneatus transmits upper limb fine touch.
Diagnosis:
Cuneate tract lesion.
Management:
Neurorehabilitation.
CASE 19: Anterior Horn Cell Tumor
Scenario:
Progressive muscle weakness with preserved sensation.
Explanation:
Motor neurons affected, sensory tracts spared.
Diagnosis:
Anterior horn tumor.
Management:
Surgical excision if operable.
CASE 20: Spinal Shock
Scenario:
Immediately after trauma, patient has flaccid paralysis and absent reflexes below lesion.
Explanation:
Transient loss of spinal reflex activity.
Diagnosis:
Spinal shock.
Management:
Supportive care; monitor recovery.
CASE 21: Recovery Phase of UMN Injury
Scenario:
Weeks after spinal injury, reflexes become exaggerated.
Explanation:
Return of reflexes with loss of cortical inhibition.
Diagnosis:
Chronic UMN lesion.
Management:
Antispastic therapy.
CASE 22: Segmental LMN Signs
Scenario:
Weakness and atrophy limited to one myotome.
Explanation:
Segmental anterior horn involvement.
Diagnosis:
Focal LMN lesion.
Management:
Physiotherapy.
CASE 23: Sensory Dissociation
Scenario:
Pain lost but touch preserved.
Explanation:
Spinothalamic damaged, dorsal column intact.
Diagnosis:
Selective spinothalamic lesion.
Management:
Treat compression.
CASE 24: Proprioceptive Ataxia
Scenario:
Patient stamps feet while walking and worsens with eyes closed.
Explanation:
Loss of dorsal column input.
Diagnosis:
Sensory ataxia.
Management:
Treat underlying cause.
CASE 25: Autonomic Dysfunction
Scenario:
Spinal injury patient has severe hypertension triggered by bladder distension.
Explanation:
Loss of descending autonomic control.
Diagnosis:
Autonomic dysreflexia.
Management:
Remove trigger, antihypertensives.
CASE 26: Hematomyelia
Scenario:
Sudden onset paraplegia with sensory loss after trauma.
Explanation:
Bleeding into spinal cord substance.
Diagnosis:
Hematomyelia.
Management:
Urgent MRI, surgical intervention.
CASE 27: Myelitis
Scenario:
Acute bilateral weakness with sensory and bladder involvement.
Explanation:
Inflammation of spinal cord affecting multiple tracts.
Diagnosis:
Transverse myelitis.
Management:
Steroids, plasma exchange.
CASE 28: Degenerative Myelopathy
Scenario:
Slowly progressive spastic paraparesis.
Explanation:
Chronic corticospinal tract degeneration.
Diagnosis:
Degenerative myelopathy.
Management:
Physiotherapy, supportive care.
CASE 29: Combined UMN and LMN Signs
Scenario:
Patient shows muscle wasting with brisk reflexes.
Explanation:
Both anterior horn and corticospinal tracts involved.
Diagnosis:
Motor neuron disease.
Management:
Multidisciplinary supportive management.
CASE 30: Complete Cord Transection
Scenario:
Total loss of motor and sensory function below lesion.
Explanation:
All ascending and descending tracts interrupted.
Diagnosis:
Complete spinal cord injury.
Management:
Emergency stabilization, rehabilitation, long-term care.