Anatomy of the Spinal Cord – Complete Guide
Location and Extent of the Spinal Cord
Location
- The spinal cord lies within the vertebral canal
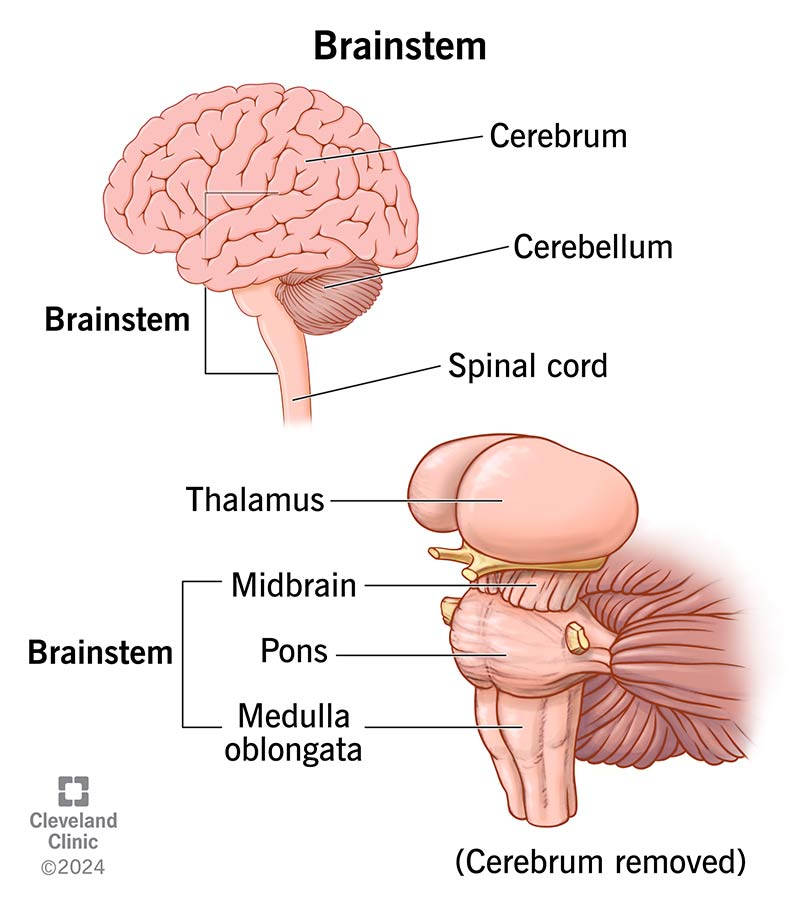
- Superiorly continuous with the medulla oblongata at the foramen magnum
- Surrounded by three meninges and cerebrospinal fluid
Extent
- Adults: Foramen magnum to L1–L2 vertebral level
- Children: Up to L2–L3
- Newborns: Up to L3–L4
Terminal Structures
- Conus medullaris: Tapered lower end of spinal cord
- Filum terminale: Fibrous extension from conus medullaris to coccyx
- Cauda equina: Collection of lumbar, sacral, and coccygeal nerve roots
Enlargements
- Cervical enlargement (C4–T1): Upper limb innervation
- Lumbosacral enlargement (L2–S3): Lower limb innervation
Meninges of the Spinal Cord and Modification of Pia Mater
Spinal Meninges
- Dura mater: Tough outer layer
- Arachnoid mater: Thin, avascular middle layer
- Pia mater: Thin, vascular layer closely adherent to cord
Modifications of Pia Mater
- Filum terminale
* Internum: Conus medullaris to S2
* Externum: S2 to coccyx
- Denticulate ligaments
* Tooth-like lateral extensions
* Anchor spinal cord to dura mater
- Linea splendens
* Thickened midline on anterior surface of cord
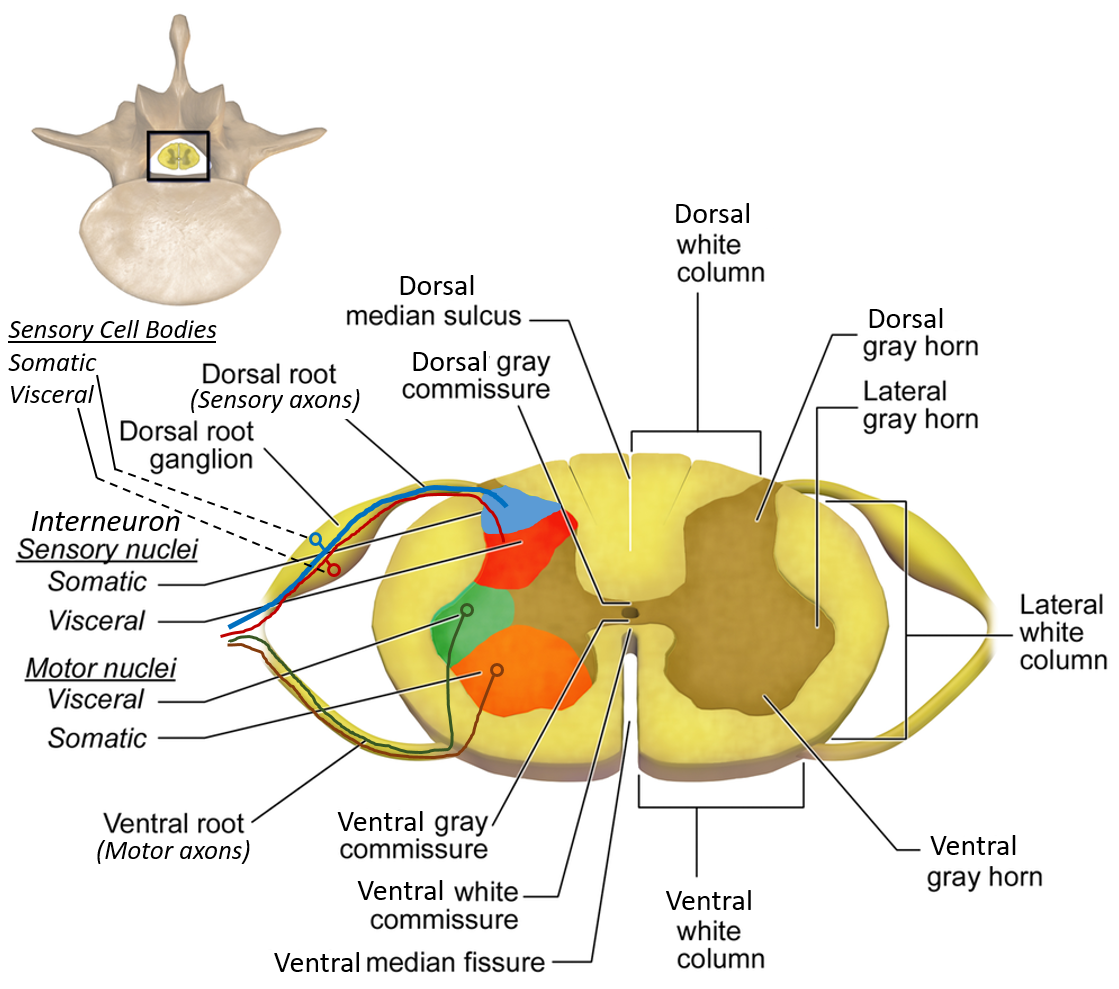
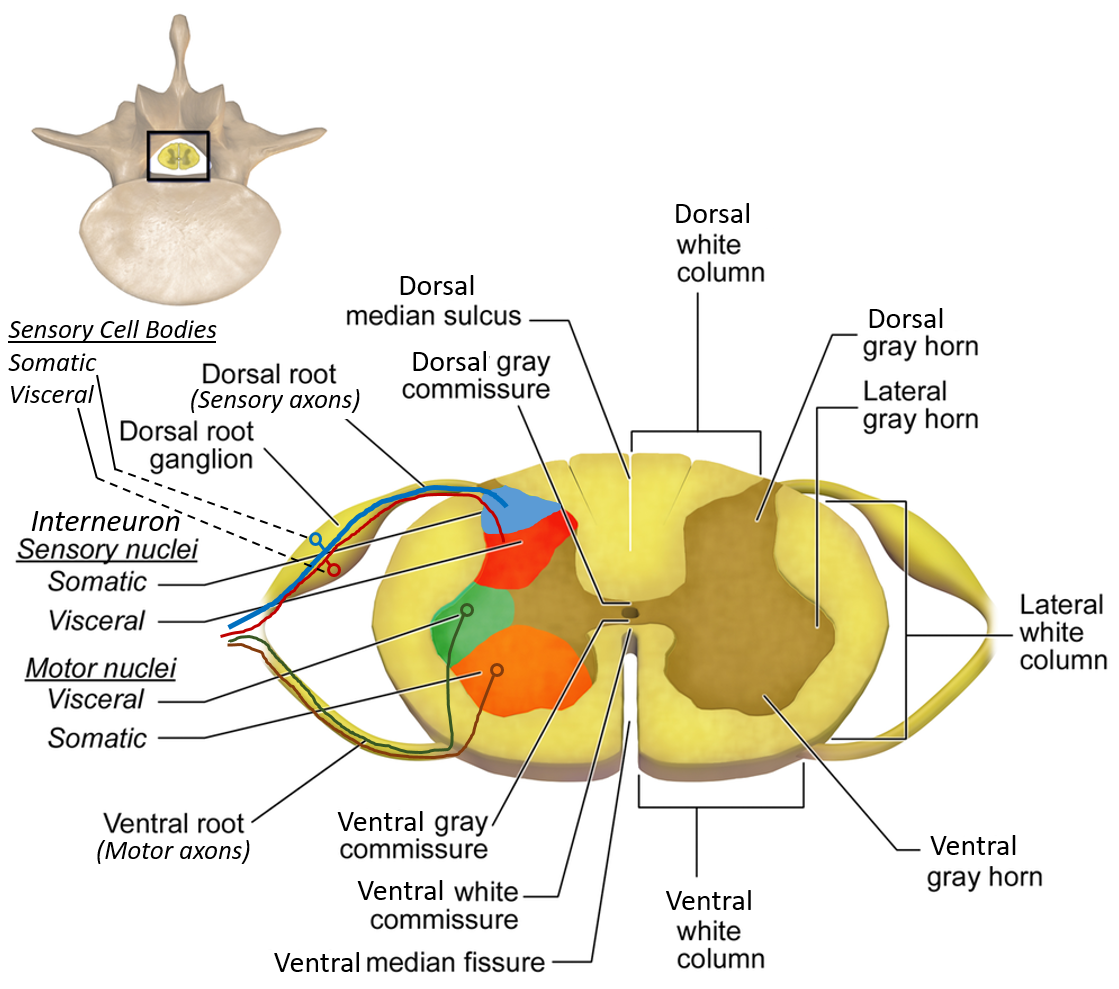
Internal Structure of the Spinal Cord
Grey Matter
- H-shaped or butterfly-shaped
- Contains neuron cell bodies
White Matter
- Surrounds grey matter
- Composed of ascending and descending tracts
Horns of the Spinal Cord
Anterior (Ventral) Horn
- Contains lower motor neurons
- Supplies skeletal muscles
- Well developed in cervical and lumbar enlargements
Posterior (Dorsal) Horn
- Sensory in function
- Receives afferent fibers from dorsal roots
Lateral Horn
- Present from T1–L2 and S2–S4
- Contains autonomic neurons
* Sympathetic (T1–L2)
* Parasympathetic (S2–S4)
Nuclei in the Grey Matter Horns
Posterior Horn Nuclei
- Substantia gelatinosa
* Pain and temperature modulation
- Nucleus proprius
* Touch and pressure
- Clarke’s column (T1–L2)
* Proprioceptive impulses to cerebellum
Anterior Horn Nuclei
- Alpha motor neurons
* Innervate extrafusal muscle fibers
- Gamma motor neurons
* Innervate muscle spindles
Lateral Horn Nuclei
- Intermediolateral cell column
* Sympathetic neurons (T1–L2)
- Sacral parasympathetic nucleus
* Parasympathetic neurons (S2–S4)
Types of Neurons
Upper Motor Neurons (UMN)
- Originate in motor cortex or brainstem
- End on lower motor neurons
- Lesion causes:
* Spastic paralysis
* Hyperreflexia
* Babinski sign
Lower Motor Neurons (LMN)
- Originate in anterior horn
- Directly innervate muscles
- Lesion causes:
* Flaccid paralysis
* Muscle wasting
* Fasciculations
Ascending Tracts of the Spinal Cord
Dorsal Column Pathway
(Fine touch, vibration, proprioception)
Components
- Fasciculus gracilis: Lower limb (below T6)
- Fasciculus cuneatus: Upper limb (above T6)
Pathway
- First-order neuron: Dorsal root ganglion
- Ascends ipsilaterally in dorsal column
- Synapse in nucleus gracilis/cuneatus (medulla)
- Decussation → medial lemniscus
- Thalamus → sensory cortex
Spinothalamic Tract
(Pain, temperature, crude touch)
Types
- Lateral spinothalamic: Pain and temperature
- Anterior spinothalamic: Crude touch and pressure
Pathway
- First-order neuron: Dorsal root ganglion
- Synapse in dorsal horn
- Decussates within 1–2 segments
- Ascends contralaterally to thalamus
- Projects to sensory cortex
Spinocerebellar Pathways
(Unconscious proprioception)
Posterior Spinocerebellar Tract
- Origin: Clarke’s column (T1–L2)
- Does not decussate
- Enters cerebellum via inferior peduncle
Anterior Spinocerebellar Tract
- Double decussation
- Enters cerebellum via superior peduncle
Descending Tracts of the Spinal Cord
Corticospinal Tract (Pyramidal)
- Lateral corticospinal: Voluntary skilled movement
- Anterior corticospinal: Axial muscles
Extrapyramidal Tracts
- Rubrospinal: Flexor facilitation
- Vestibulospinal: Posture and balance
- Reticulospinal: Muscle tone and reflexes
- Tectospinal: Head and neck reflexes
UMN and LMN Pathways
Upper Motor Neuron Pathway
- Motor cortex → internal capsule → brainstem → spinal cord
- Controls voluntary movement
Lower Motor Neuron Pathway
- Anterior horn → peripheral nerve → muscle
- Final common pathway for motor activity
Clinical Importance
- Brown-Sequard syndrome: Hemisection of cord
- Syringomyelia: Central cord lesion
- Tabes dorsalis: Dorsal column degeneration
- ALS: Combined UMN and LMN degeneration
If you want, I can:
- Convert this into MCQs
- Create exam-oriented tables
- Generate HTML-CSS-JS medical notes
- Add SEO title, description, keywords, FAQ schema
Just tell me 👍
Below are 30 detailed, exam-oriented clinical case scenarios related to spinal cord anatomy, each followed by diagnosis reasoning and management.
Structured for SEO, medical exams (UG + PG), and clinical correlation.
Spinal Cord Anatomy – 30 Clinical Case Scenarios With Management
CASE 1: Cervical Cord Compression
Scenario:
A 45-year-old man presents with neck pain, weakness of all four limbs, hyperreflexia, and difficulty walking.
Likely Diagnosis: Cervical myelopathy
Anatomical Basis: Compression of cervical spinal cord affecting corticospinal tracts
Management:
- MRI cervical spine
- Cervical immobilization
- Surgical decompression (laminectomy)
- Physiotherapy and rehabilitation
CASE 2: Brown-Sequard Syndrome
Scenario:
A stab injury to the right side of spinal cord at T10 causes ipsilateral motor loss and contralateral pain loss.
Diagnosis: Brown-Sequard syndrome
Anatomy:
- Ipsilateral corticospinal & dorsal column damage
- Contralateral spinothalamic loss
Management:
- Stabilize spine
- High-dose steroids (acute)
- Surgical repair if required
- Neurorehabilitation
CASE 3: Syringomyelia
Scenario:
Young adult with bilateral loss of pain and temperature over shoulders and arms.
Diagnosis: Syringomyelia
Anatomy: Central canal expansion damaging spinothalamic decussation
Management:
- MRI cervical spine
- Treat underlying cause (Chiari malformation)
- Surgical shunting
CASE 4: Tabes Dorsalis
Scenario:
Patient with ataxic gait, loss of vibration sense, positive Romberg.
Diagnosis: Dorsal column degeneration (Tabes dorsalis)
Anatomy: Fasciculus gracilis and cuneatus
Management:
- VDRL/TPHA testing
- IV penicillin
- Supportive gait training
CASE 5: ALS (Motor Neuron Disease)
Scenario:
Progressive weakness, muscle wasting, hyperreflexia.
Diagnosis: Amyotrophic lateral sclerosis
Anatomy: UMN + LMN degeneration
Management:
- Riluzole
- Respiratory support
- Multidisciplinary care
CASE 6: Acute Transverse Myelitis
Scenario:
Sudden paraplegia with sensory level at T8.
Diagnosis: Transverse myelitis
Anatomy: Entire cord segment inflammation
Management:
- IV methylprednisolone
- Plasma exchange
- Treat underlying infection/autoimmune cause
CASE 7: Cauda Equina Syndrome
Scenario:
Low back pain, saddle anesthesia, bladder dysfunction.
Diagnosis: Cauda equina syndrome
Anatomy: Compression of nerve roots below conus
Management:
- Emergency MRI
- Surgical decompression
- Bladder catheterization
CASE 8: Conus Medullaris Syndrome
Scenario:
Early bladder dysfunction, mild leg weakness.
Diagnosis: Conus medullaris lesion
Anatomy: Terminal spinal cord
Management:
- MRI spine
- Treat tumor/inflammation
- Bowel and bladder care
CASE 9: Poliomyelitis
Scenario:
Child with acute flaccid paralysis and absent reflexes.
Diagnosis: Anterior horn cell disease
Anatomy: LMN destruction
Management:
- Supportive care
- Physiotherapy
- Vaccination prevention
CASE 10: Cervical Disc Prolapse
Scenario:
Radicular pain with UMN signs in legs.
Diagnosis: Cervical disc herniation
Anatomy: Cord and nerve root compression
Management:
- MRI
- Conservative therapy
- Surgical discectomy
CASE 11: Thoracic Cord Tumor
Scenario:
Progressive spastic paraplegia with sensory level.
Diagnosis: Intramedullary tumor
Management:
- MRI
- Surgical excision
- Radiotherapy if indicated
CASE 12: Lumbar Spinal Stenosis
Scenario:
Neurogenic claudication relieved by flexion.
Diagnosis: Lumbar canal stenosis
Anatomy: Compression of cauda equina
Management:
- NSAIDs
- Physiotherapy
- Decompression surgery
CASE 13: Posterior Column Lesion
Scenario:
Loss of vibration and joint position sense.
Diagnosis: Dorsal column injury
Management:
- Treat cause (B12 deficiency, syphilis)
- Vitamin replacement
CASE 14: Spinothalamic Tract Lesion
Scenario:
Contralateral pain loss starting 2 segments below lesion.
Diagnosis: Spinothalamic tract damage
Management:
- Identify etiology
- Symptomatic pain control
CASE 15: Multiple Sclerosis
Scenario:
Young woman with episodic weakness and sensory symptoms.
Diagnosis: MS
Anatomy: Demyelination of spinal tracts
Management:
- Steroids for relapse
- Disease-modifying therapy
CASE 16: Epidural Abscess
Scenario:
Fever, back pain, rapidly progressing paraplegia.
Diagnosis: Spinal epidural abscess
Management:
- Emergency MRI
- IV antibiotics
- Surgical drainage
CASE 17: Vertebral Fracture
Scenario:
Trauma with sudden paraplegia.
Diagnosis: Spinal cord injury
Management:
- Immobilization
- Surgical stabilization
- Rehabilitation
CASE 18: Autonomic Dysreflexia
Scenario:
T6 lesion with sudden hypertension and sweating.
Diagnosis: Autonomic dysreflexia
Management:
- Sit patient upright
- Remove trigger (bladder, bowel)
- Antihypertensives
CASE 19: Anterior Spinal Artery Syndrome
Scenario:
Motor paralysis with preserved dorsal column sensation.
Diagnosis: Anterior spinal artery infarct
Management:
- Supportive care
- Manage vascular risk factors
CASE 20: Friedreich Ataxia
Scenario:
Teenager with progressive gait ataxia.
Diagnosis: Spinocerebellar tract degeneration
Management:
- Genetic counseling
- Supportive therapy
CASE 21: Vitamin B12 Deficiency
Scenario:
Ataxia, paresthesia, anemia.
Diagnosis: Subacute combined degeneration
Anatomy: Dorsal column + corticospinal
Management:
- Vitamin B12 injections
CASE 22: Pott’s Spine
Scenario:
Back pain, gibbus deformity, paraplegia.
Diagnosis: Spinal tuberculosis
Management:
- Anti-tubercular therapy
- Surgical decompression if severe
CASE 23: Intradural Extramedullary Tumor
Scenario:
Slowly progressive weakness with radicular pain.
Diagnosis: Meningioma or schwannoma
Management:
- MRI
- Surgical excision
CASE 24: Acute Spinal Shock
Scenario:
Flaccid paralysis immediately after trauma.
Diagnosis: Spinal shock
Management:
- Supportive
- Monitor recovery of reflexes
CASE 25: Lateral Medullary Extension
Scenario:
Loss of pain and temperature in body with cranial nerve involvement.
Diagnosis: Spinothalamic tract involvement
Management:
- Treat vascular cause
CASE 26: Hereditary Spastic Paraplegia
Scenario:
Gradual progressive spasticity of legs.
Diagnosis: UMN tract degeneration
Management:
- Antispastic drugs
- Physiotherapy
CASE 27: Sacral Parasympathetic Lesion
Scenario:
Urinary retention and erectile dysfunction.
Diagnosis: S2–S4 lesion
Management:
- Bladder training
- Treat underlying lesion
CASE 28: Central Cord Syndrome
Scenario:
Greater weakness in upper limbs than lower limbs.
Diagnosis: Central cervical cord injury
Management:
- Immobilization
- Steroids
- Surgery if needed
CASE 29: Posterior Spinocerebellar Tract Lesion
Scenario:
Ipsilateral limb ataxia without weakness.
Diagnosis: Spinocerebellar tract lesion
Management:
- Treat underlying cause
- Rehabilitation
CASE 30: Complete Spinal Cord Transection
Scenario:
Total motor and sensory loss below lesion.
Diagnosis: Complete spinal cord injury
Management:
- Acute stabilization
- Long-term rehabilitation
- Prevent complications