SHOCK
1. Definition
Shock is a life-threatening clinical syndrome in which there is:
- Inadequate tissue perfusion
- Reduced oxygen delivery
- Cellular hypoxia
- Organ dysfunction
It results in circulatory failure and can rapidly progress to multi-organ failure and death if untreated.
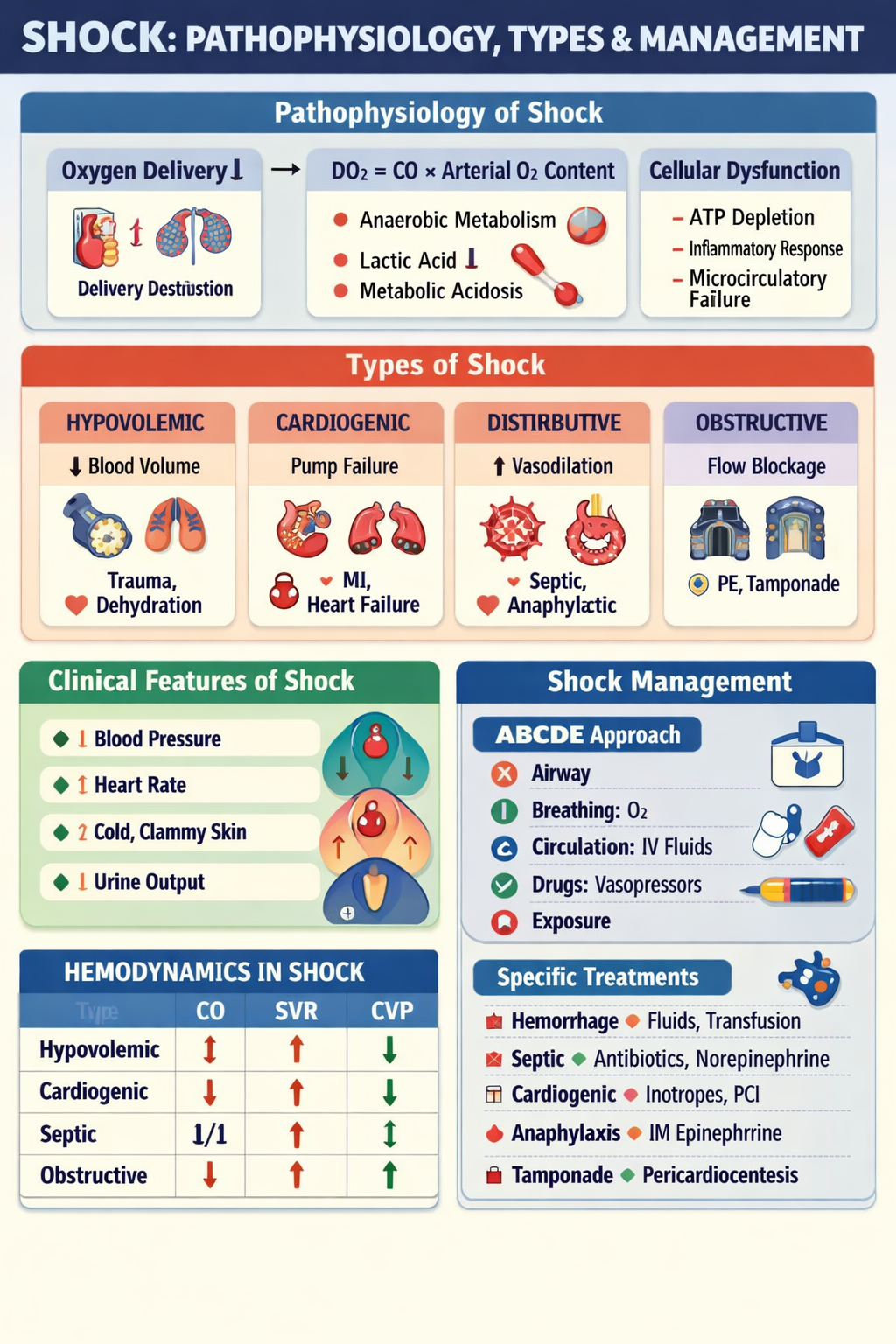
2. Pathophysiology of Shock
Shock is fundamentally a problem of oxygen supply–demand mismatch.
A. Primary Problem
↓ Effective circulation → ↓ Tissue perfusion → ↓ Oxygen delivery
B. Oxygen Delivery Equation
[
DO_2 = Cardiac\ Output \times Arterial\ Oxygen\ Content
]
So shock occurs due to:
- ↓ Cardiac output
OR
- ↓ Oxygen content
OR
- Maldistribution of blood flow
C. Cellular and Metabolic Changes
1. Anaerobic Metabolism
When oxygen is insufficient:
- Cells shift from aerobic to anaerobic metabolism
- Produces lactic acid
→ Metabolic acidosis
2. ATP Depletion
- Failure of Na⁺/K⁺ ATPase pump
- Cellular swelling
- Membrane dysfunction
3. Inflammatory Cascade
Shock activates systemic inflammation:
- Cytokines (TNF-α, IL-1)
- Nitric oxide release
- Capillary leak
→ worsens hypotension and edema
4. Microcirculatory Failure
Even if BP is restored, tissue perfusion may remain impaired due to:
- Endothelial injury
- Capillary thrombosis
- Sludging of blood
D. Stages of Shock
1. Compensated (Early Shock)
Body maintains BP by:
- Tachycardia
- Vasoconstriction
- Renin-angiotensin activation
Signs:
- Cold extremities
- Anxiety
- Mild hypotension or normal BP
2. Progressive Shock
Compensation fails:
- Hypotension develops
- Confusion
- Oliguria
- Rising lactate
3. Irreversible Shock
Severe cellular injury:
- Multi-organ failure
- Refractory hypotension
- Death despite therapy
3. Types of Shock
Shock is classified based on the main hemodynamic defect.
1. Hypovolemic Shock
Cause
Loss of circulating volume:
- Hemorrhage (trauma, GI bleed)
- Dehydration (vomiting, diarrhea)
- Burns (plasma loss)
Pathophysiology
↓ Preload → ↓ Stroke volume → ↓ Cardiac output
Clinical Features
- Tachycardia
- Hypotension
- Cold clammy skin
- Collapsed veins
- Low urine output
Hemodynamics
- ↓ CVP
- ↓ Cardiac output
- ↑ SVR (vasoconstriction)
2. Cardiogenic Shock
Cause
Pump failure:
- Acute myocardial infarction
- Severe heart failure
- Arrhythmias
- Myocarditis
Pathophysiology
Heart cannot pump effectively:
↓ Cardiac output despite normal volume
→ pulmonary congestion + systemic hypoperfusion
Clinical Features
- Hypotension
- Pulmonary edema
- Raised JVP
- Cold extremities
Hemodynamics
- ↑ CVP
- ↓ Cardiac output
- ↑ SVR
3. Distributive Shock
Main problem: Peripheral vasodilation → maldistribution of blood
Includes:
A. Septic Shock
Due to infection and systemic inflammation.
Mechanisms:
- Vasodilation (NO mediated)
- Capillary leak
- Myocardial depression
Signs:
- Warm flushed skin early
- Fever
- Hypotension
Hemodynamics:
- ↓ SVR
- Normal or ↑ CO early
B. Anaphylactic Shock
IgE-mediated allergic reaction.
Mechanisms:
- Massive histamine release
- Vasodilation
- Bronchospasm
Signs:
- Urticaria
- Wheezing
- Facial swelling
C. Neurogenic Shock
Loss of sympathetic tone (spinal injury).
Signs:
- Hypotension
- Bradycardia (unique)
- Warm dry skin
Hemodynamics:
- ↓ SVR
- ↓ HR
4. Obstructive Shock
Mechanical obstruction to circulation.
Causes
- Pulmonary embolism
- Cardiac tamponade
- Tension pneumothorax
Pathophysiology
Obstruction → ↓ Venous return or ↓ Cardiac output
Clinical Features
- Hypotension
- Raised JVP
- Clear lungs (tamponade) or absent breath sounds (pneumothorax)
Hemodynamics
- ↑ CVP
- ↓ CO
- ↑ SVR
4. Clinical Features of Shock (General)
Vital Signs
- Hypotension
- Tachycardia (except neurogenic)
- Tachypnea
Signs of Poor Perfusion
- Cold clammy skin (except early septic)
- Delayed capillary refill
- Confusion
- Oliguria (<0.5 mL/kg/hr)
Laboratory
- Raised lactate
- Metabolic acidosis
- Organ dysfunction markers (creatinine, LFTs)
5. Management of Shock (Stepwise)
Management depends on cause, but initial approach is universal.
A. Immediate Resuscitation: ABCDE
A – Airway
- Secure airway
- Consider intubation if unconscious
B – Breathing
- High-flow oxygen
- Maintain SpO₂ > 94%
C – Circulation
- 2 large-bore IV cannulas
- Monitor BP, HR, ECG
Fluid Resuscitation
- Crystalloids (Normal saline or Ringer lactate)
Typical bolus:
- Adults: 500–1000 mL rapid
- Children: 20 mL/kg
Vasopressors (if hypotension persists)
Norepinephrine (First line in septic shock)
- Strong α1 vasoconstriction
- Dose: 0.05–1 µg/kg/min
Epinephrine
Used in anaphylaxis and refractory shock.
Dopamine
Sometimes used if bradycardic hypotension.
D – Disability
- Check GCS
- Blood glucose
E – Exposure
- Look for bleeding, rash, trauma
6. Cause-Specific Management
Hypovolemic Shock
- Control bleeding
- Rapid IV fluids
- Blood transfusion if hemorrhage
- Surgery if internal bleeding
Cardiogenic Shock
Avoid excessive fluids.
Treatment:
- Inotropes (Dobutamine)
- Vasopressors if severe hypotension
- Revascularization (PCI for MI)
- Mechanical support (IABP/ECMO)
Septic Shock
- Early broad-spectrum antibiotics (within 1 hour)
- IV fluids (30 mL/kg)
- Norepinephrine if MAP <65 mmHg
- Source control (drain abscess)
Anaphylactic Shock
First line: IM Epinephrine
Dose:
- Adults: 0.5 mg IM (1:1000)
- Children: 0.01 mg/kg IM
Also:
- Antihistamines
- Steroids
- Bronchodilators
Obstructive Shock
Treat obstruction:
- Tamponade → Pericardiocentesis
- Tension pneumothorax → Needle decompression
- PE → Thrombolysis or embolectomy
7. Monitoring and Endpoints
Goals:
- MAP ≥ 65 mmHg
- Urine output ≥ 0.5 mL/kg/hr
- Lactate clearance
- Normal mental status
Monitoring:
- ECG
- ABG
- Lactate
- Central venous pressure (selected cases)
8. Complications of Shock
- Acute kidney injury
- ARDS
- DIC
- Multi-organ failure
- Death
Summary Table
| Type | Main Defect | CO | SVR | CVP |
| ------------ | ------------------------ | --- | --- | -------- |
| Hypovolemic | Volume loss | ↓ | ↑ | ↓ |
| Cardiogenic | Pump failure | ↓ | ↑ | ↑ |
| Septic | Vasodilation | ↑/↓ | ↓ | Normal/↓ |
| Anaphylactic | Vasodilation + leak | ↓ | ↓ | ↓ |
| Neurogenic | Loss of sympathetic tone | ↓ | ↓ | ↓ |
| Obstructive | Mechanical block | ↓ | ↑ | ↑ |