**Hyperaldosteronism —
Definition
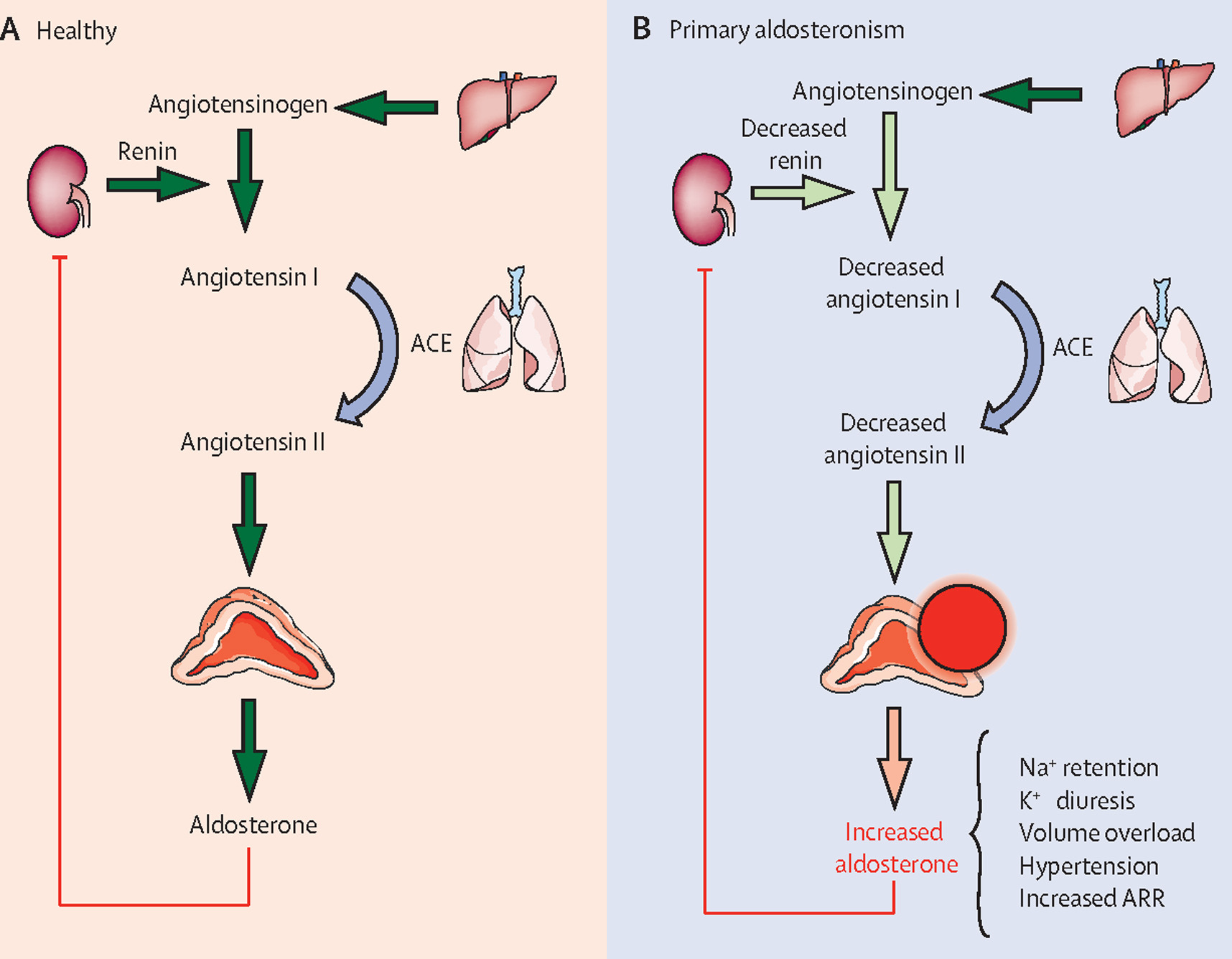
Hyperaldosteronism is a disorder characterized by excessive production of aldosterone by the adrenal cortex, leading to sodium and water retention, potassium loss, metabolic alkalosis, and suppressed renin activity (in primary forms).
Physiology of Aldosterone (Brief)
- Secreted from zona glomerulosa
- Regulated mainly by RAAS, serum potassium, and ACTH (minor role)
- Acts on distal tubules and collecting ducts
* ↑ Na⁺ reabsorption
* ↑ K⁺ and H⁺ secretion
* ↑ intravascular volume → hypertension
Classification
1. Primary Hyperaldosteronism (PA)
Autonomous aldosterone secretion, low renin
Causes
- Aldosterone-producing adenoma (Conn syndrome) – most common
- Bilateral adrenal hyperplasia
- Unilateral adrenal hyperplasia
- Familial hyperaldosteronism (Types I–IV)
- Rare: adrenal carcinoma
2. Secondary Hyperaldosteronism
RAAS-driven, high renin
Causes
- Renal artery stenosis
- Congestive heart failure
- Cirrhosis with ascites
- Nephrotic syndrome
- Diuretic use
- Renin-secreting tumors
- Pregnancy
3. Pseudohyperaldosteronism
Aldosterone-like effects without elevated aldosterone
- Liddle syndrome
- Apparent mineralocorticoid excess
- Licorice ingestion (glycyrrhizin)
Pathophysiology
- Excess aldosterone → ENaC overactivation
- ↑ Sodium reabsorption → plasma volume expansion
- ↓ Potassium → hypokalemia
- ↑ H⁺ excretion → metabolic alkalosis
- Suppression of renin (primary forms)
- Long-term effects: vascular remodeling, LV hypertrophy, fibrosis
Clinical Features
Cardinal Features
- Hypertension (often resistant)
- Hypokalemia (may be absent in early disease)
Symptoms of Hypokalemia
- Muscle weakness, cramps
- Fatigue
- Polyuria, polydipsia
- Paresthesias
- Paralysis (severe)
Cardiac Manifestations
- Arrhythmias
- Left ventricular hypertrophy
- Increased CV morbidity independent of BP
Others
- Metabolic alkalosis
- No edema (aldosterone escape)
Indications to Screen
Screen all patients with:
- Resistant hypertension (≥3 drugs)
- Hypertension with hypokalemia
- Hypertension with adrenal incidentaloma
- Early-onset hypertension (<40 years)
- Hypertension + family history of PA or stroke <40
- Severe hypertension (>150/100 mmHg)
Investigations
1. Screening Test
Plasma Aldosterone-Renin Ratio (ARR)
| Parameter | Finding in Primary Hyperaldosteronism |
| ----------- | ------------------------------------- |
| Aldosterone | High |
| Renin | Suppressed |
| ARR | Elevated |
> Drugs affecting ARR: ACE inhibitors, ARBs, diuretics, beta-blockers
> Preferred agents during testing: verapamil, hydralazine, α-blockers
2. Confirmatory Tests (Any one)
- Saline infusion test
- Oral sodium loading test
- Fludrocortisone suppression test
- Captopril challenge test
Failure to suppress aldosterone confirms PA
3. Subtype Differentiation
- CT/MRI adrenal glands
- Adrenal venous sampling (AVS) – gold standard
(mandatory before surgery unless young patient with clear unilateral adenoma)
4. Additional Tests
- Serum electrolytes
- ABG (metabolic alkalosis)
- ECG (U waves)
- Echocardiography (LVH)
Differential Diagnosis
- Essential hypertension
- Renal artery stenosis
- Cushing syndrome
- Liddle syndrome
- Apparent mineralocorticoid excess
- Chronic kidney disease
- Diuretic abuse
Management
A. Primary Hyperaldosteronism
1. Unilateral Disease (Adenoma / Unilateral Hyperplasia)
Definitive treatment
- Laparoscopic adrenalectomy
Outcomes
- Cure or improvement of hypertension
- Normalization of potassium
- Reduced CV risk
2. Bilateral Adrenal Hyperplasia
Medical therapy preferred
B. Secondary Hyperaldosteronism
- Treat underlying cause (e.g., revascularization for renal artery stenosis, HF optimization)
- Mineralocorticoid receptor antagonists if needed
Pharmacologic Therapy (Detailed)
1. Spironolactone
Indication
- First-line for bilateral PA
Mechanism
- Competitive aldosterone receptor antagonist
Dose
- Adult: 12.5–50 mg/day (up to 400 mg/day if needed)
- Pediatric: 1–3 mg/kg/day
Pharmacokinetics
- Oral
- Hepatic metabolism
- Active metabolites (canrenone)
Adverse Effects
- Hyperkalemia
- Gynecomastia
- Menstrual irregularities
- Decreased libido
- GI upset
Contraindications
- Hyperkalemia
- Severe renal failure
Drug Interactions
- ACE inhibitors, ARBs
- Potassium supplements
- NSAIDs
Monitoring
- Serum potassium
- Renal function
Patient Counselling
- Avoid potassium-rich salt substitutes
- Report breast tenderness or menstrual changes
2. Eplerenone
Indication
- Alternative to spironolactone (fewer endocrine side effects)
Mechanism
- Selective mineralocorticoid receptor antagonist
Dose
- Adult: 25–50 mg twice daily
Adverse Effects
- Hyperkalemia (less gynecomastia)
Contraindications
- Severe renal impairment
- CYP3A4 inhibitors
3. Amiloride
Indication
- Pseudohyperaldosteronism or intolerance to MR antagonists
Mechanism
- ENaC blocker
Dose
- Adult: 5–20 mg/day
Adverse Effects
- Hyperkalemia
Non-Pharmacologic Measures
- Dietary sodium restriction
- BP control lifestyle measures
- Avoid licorice products
- Regular electrolyte monitoring
Special Situations
Pregnancy
- Avoid spironolactone
- Preferred: amiloride, eplerenone (with caution)
Familial Hyperaldosteronism Type I
- Glucocorticoid-remediable
- Low-dose dexamethasone suppresses ACTH
Complications
- Stroke
- Myocardial infarction
- Atrial fibrillation
- Chronic kidney disease
- Sudden cardiac death
Prognosis
- Excellent with early diagnosis
- Surgery offers potential cure
- Medical therapy significantly reduces CV risk
Key Exam Pearls
- Normal potassium does not exclude hyperaldosteronism
- PA is the most common cause of secondary hypertension
- AVS is required before surgery
- Aldosterone causes hypertension without edema