HIGH-ALTITUDE PULMONARY EDEMA (HAPE)
1. Definition
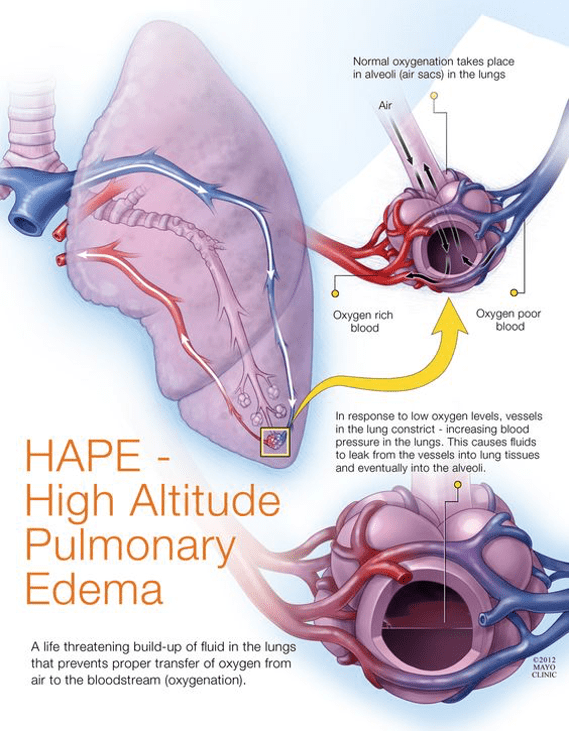
High-Altitude Pulmonary Edema (HAPE) is a life-threatening, non-cardiogenic pulmonary edema that occurs due to hypoxia-induced pulmonary hypertension after rapid ascent to high altitude, usually >2,500–3,000 m.
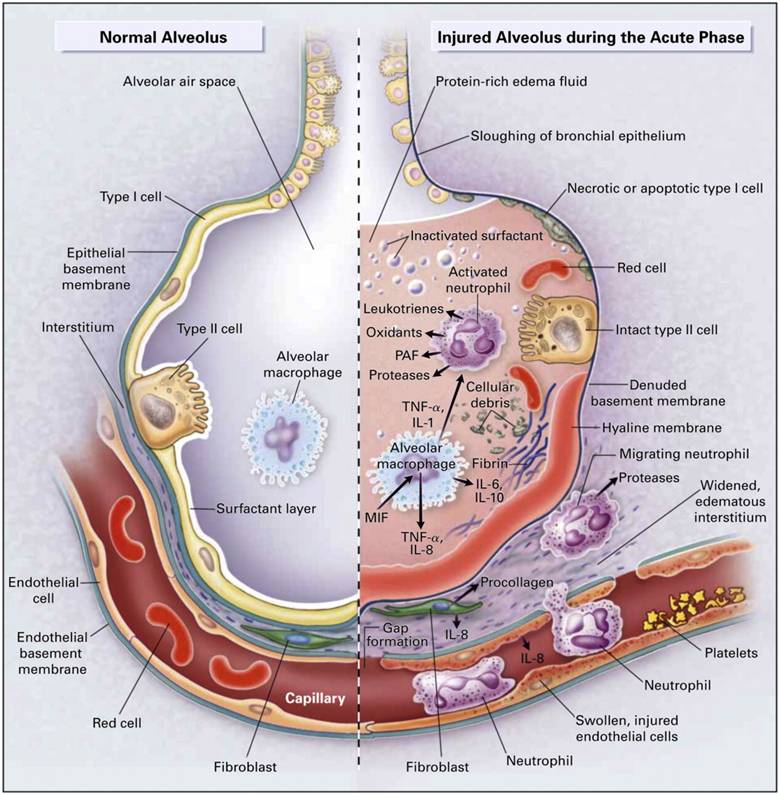
2. Pathophysiology
- Hypobaric hypoxia → uneven hypoxic pulmonary vasoconstriction
- Over-perfusion of some capillary beds → capillary stress failure
- Leakage of protein-rich fluid into alveoli
- No left ventricular dysfunction (normal PCWP)
- Reduced nitric oxide, increased endothelin-1
- Genetic susceptibility (↓ HIF response)
3. Risk Factors / Triggers
- Rapid ascent
- No acclimatization
- Prior history of HAPE
- Cold exposure
- Heavy exertion
- Respiratory infection
- Male sex
- Use of sedatives or alcohol
4. Clinical Features
Early Symptoms
- Reduced exercise tolerance
- Dry cough
- Dyspnea on exertion
- Fatigue
Progressive / Severe Features
- Dyspnea at rest
- Orthopnea
- Pink frothy sputum
- Chest tightness
- Cyanosis
- Tachycardia, tachypnea
- Low-grade fever (misleading)
Examination
- Crackles (often right middle/lower lobe first)
- Wheeze
- Hypoxia disproportionate to exam
5. Investigations
At Altitude (Clinical Diagnosis)
- SpO₂ markedly reduced
- Chest auscultation: crackles
- Portable CXR (if available): patchy perihilar opacities
Hospital
- Chest X-ray: bilateral patchy infiltrates, normal heart size
- ABG: hypoxemia ± respiratory alkalosis
- Echocardiography: elevated pulmonary artery pressure, normal LV
- BNP: normal or mildly elevated
6. Differential Diagnosis
- Pneumonia
- Pulmonary embolism
- Acute mountain sickness (AMS)
- High-altitude cerebral edema (HACE)
- Cardiogenic pulmonary edema
- ARDS
7. Management (Stepwise)
Immediate (Life-Saving)
- Immediate descent (≥1,000 m) → MOST IMPORTANT
- High-flow oxygen (target SpO₂ >90%)
- Rest and warmth
Pharmacologic Management
A. Nifedipine
- Indication: Moderate–severe HAPE, prevention in high-risk
- Mechanism: Pulmonary vasodilation → ↓ pulmonary artery pressure
- Dose:
* Adult: 30 mg SR PO every 12 hours
- Adverse Effects: Hypotension, headache, flushing
- Contraindications: Hypotension
- Monitoring: BP
- Counseling: Rise slowly, avoid dehydration
B. Phosphodiesterase-5 Inhibitors (Adjunct)
- Sildenafil: 50 mg PO every 8 hours
- Tadalafil: 10 mg PO twice daily
- MOA: ↑ NO-mediated vasodilation
- Avoid with nitrates
C. Dexamethasone (If HACE overlap)
- 8 mg loading → 4 mg every 6 hours
Non-Pharmacologic
- Portable hyperbaric chamber (Gamow bag)
- Avoid exertion
- Avoid alcohol/sedatives
8. Prevention
- Gradual ascent (<300–500 m/day above 3,000 m)
- Rest days every 1,000 m
- Nifedipine prophylaxis in prior HAPE
- Avoid cold exposure
- Adequate hydration
9. Prognosis
- Excellent with early descent
- Fatal if untreated
- High recurrence risk without prevention
HYPOTHERMIA
1. Definition
Hypothermia is a condition where core body temperature <35°C (95°F) due to failure of thermoregulation.
2. Classification
| Severity | Core Temperature |
| -------- | ---------------- |
| Mild | 32–35°C |
| Moderate | 28–32°C |
| Severe | <28°C |
3. Pathophysiology
- Heat loss > heat production
- Peripheral vasoconstriction → heat conservation
- ↓ Enzyme activity
- Cardiac electrical instability
- Coagulopathy
- Cold diuresis → hypovolemia
4. Causes
Environmental
- Cold exposure
- Immersion in cold water
- High altitude
Medical
- Sepsis
- Hypothyroidism
- Adrenal insufficiency
- Malnutrition
Drugs
- Alcohol
- Sedatives
- Antipsychotics
- Opioids
5. Clinical Features
Mild (32–35°C)
- Shivering
- Tachycardia
- Slurred speech
- Ataxia
Moderate (28–32°C)
- Cessation of shivering
- Bradycardia
- Hypotension
- Altered sensorium
Severe (<28°C)
- Coma
- Ventricular arrhythmias
- Apnea
- Fixed pupils (can be reversible)
6. Investigations
- Core temperature (esophageal, rectal, bladder)
- ECG: Osborn (J) waves, prolonged PR/QT
- ABG: metabolic acidosis
- Electrolytes (hypokalemia initially)
- Coagulation profile
- Glucose (hypoglycemia common)
7. Differential Diagnosis
- Stroke
- Drug overdose
- Sepsis
- Hypoglycemia
- Myxedema coma
8. Management (Stepwise)
General Principles
- Handle gently (prevent arrhythmias)
- ABC stabilization
- Treat hypoglycemia
- “No one is dead until warm and dead”
A. Passive Rewarming (Mild)
- Remove wet clothes
- Insulation
- Warm environment
- Oral warm fluids (if conscious)
B. Active External Rewarming (Moderate)
- Forced warm air blankets
- Heating pads to trunk (not limbs)
- Warm IV fluids (38–42°C)
C. Active Internal Rewarming (Severe)
- Warm IV fluids
- Warm humidified oxygen
- Gastric, bladder, peritoneal lavage
- ECMO / cardiopulmonary bypass (gold standard if cardiac arrest)
9. Cardiac Arrest in Hypothermia
- Prolonged CPR allowed
- Defibrillation ≤3 attempts until temp >30°C
- Medications withheld or spaced widely <30°C
10. Complications
- Ventricular fibrillation
- Coagulopathy
- Rhabdomyolysis
- Acute kidney injury
- Aspiration pneumonia
11. Prognosis
- Excellent with timely rewarming
- Children and cold-water immersion have better outcomes
- Survival reported at core temps as low as 13.7°C
12. Key Exam Pearls
- HAPE = descent + oxygen
- Hypothermia = gentle handling
- Shivering stops at ~30°C
- Osborn waves are characteristic
- Do not declare death until rewarmed