Second Heart Sound (S2)
Definition
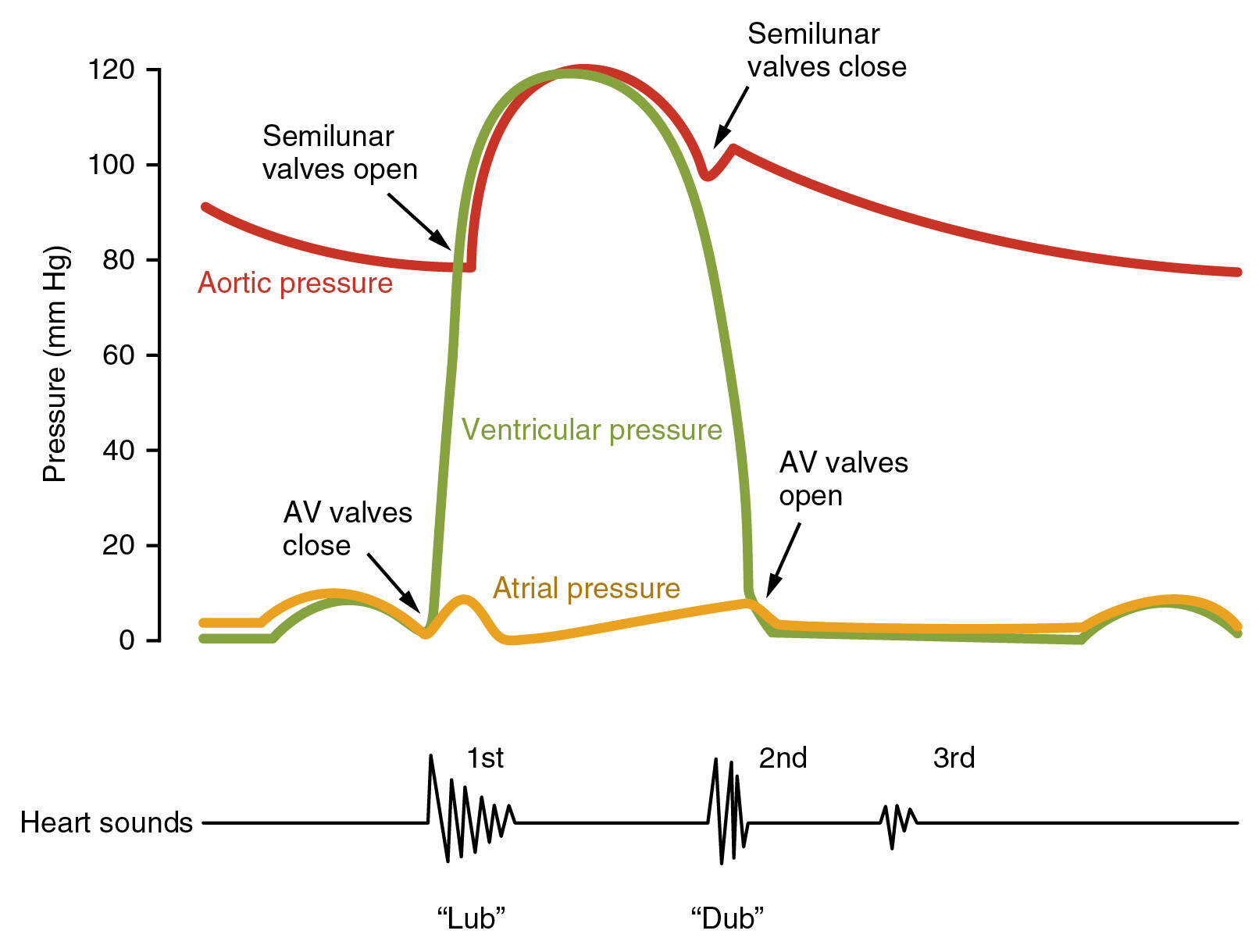
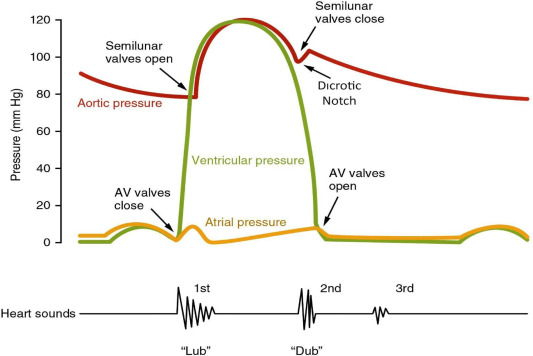
Second heart sound (S2) is the high-frequency heart sound produced by closure of the semilunar valves:
- A2 – Aortic valve closure
- P2 – Pulmonary valve closure
It marks the end of ventricular systole and beginning of diastole.
Physiology & Mechanism
- As ventricular pressure falls below great artery pressure:
* Aortic valve closes → A2
* Pulmonary valve closes → P2
- Normally A2 precedes P2 due to:
* Higher systemic pressure
* Shorter LV ejection time
- Best heard with diaphragm of stethoscope.
Auscultation Areas
- A2: Right 2nd intercostal space (aortic area)
- P2: Left 2nd intercostal space (pulmonary area)
Normal Splitting of S2
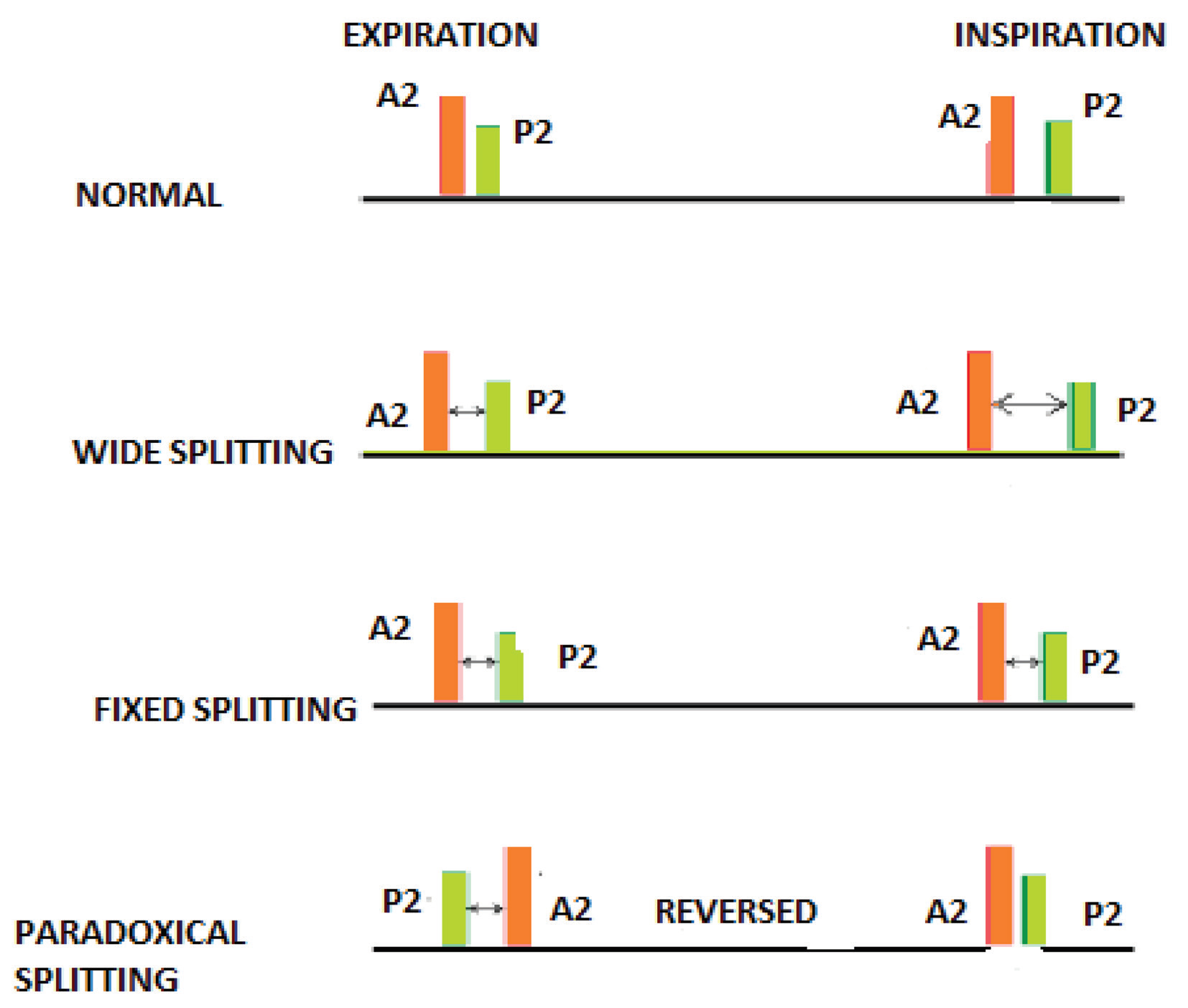
Physiological splitting occurs during inspiration:
- Increased venous return → delayed RV emptying → delayed P2
- Expiration → split narrows or disappears
Abnormal Splitting Patterns (High-Yield)
1. Wide Splitting
- Increased separation in inspiration, persists in expiration
- Causes:
* Right bundle branch block (RBBB)
* Pulmonary stenosis
* Pulmonary embolism
2. Fixed Splitting
- No respiratory variation
- Classic cause:
* Atrial septal defect (ASD)
3. Paradoxical (Reversed) Splitting
- Split heard during expiration, disappears in inspiration
- Mechanism: delayed A2
- Causes:
* Left bundle branch block (LBBB)
* Severe aortic stenosis
* Hypertrophic cardiomyopathy
Intensity Changes of S2 Components
A2
- Loud A2:
* Systemic hypertension
- Soft/Absent A2:
* Severe aortic stenosis
* Aortic regurgitation
P2
- Loud P2 (Accentuated):
* Pulmonary hypertension
* Mitral stenosis (late)
- Soft/Absent P2:
* Pulmonary stenosis
Clinical Correlations
- Single S2:
* Severe aortic stenosis
* Severe pulmonary stenosis
- Palpable P2:
* Suggests pulmonary hypertension
- Split S2 best heard in pulmonary area
Timing & Differentiation
| Feature | S2 |
| --------------- | ----------------- |
| Phase | Start of diastole |
| Pitch | High |
| Best heard with | Diaphragm |
| Compared to S1 | Shorter, sharper |
Special Clinical Situations
- Pulmonary hypertension → loud, sharp P2
- ASD → fixed wide splitting
- LBBB → paradoxical splitting
- Severe AS → soft or absent A2
Examination Pearls
- Always assess splitting with respiration
- Compare A2 vs P2 intensity
- A loud P2 is a marker of pulmonary arterial pressure
- Fixed split S2 = ASD until proven otherwise
One-Line Summary
S2 represents closure of aortic and pulmonary valves; its splitting pattern and intensity provide critical clues to conduction defects, valvular disease, and pulmonary hypertension.
If you want, I can also provide:
- Hard exam MCQs (case-based)
- Comparison table: S1 vs S2 vs S3 vs S4
- Clinical viva questions
- Heart sounds auscultation algorithm
Below are HARD, EXAM-ORIENTED, ALL-POSSIBLE CASE SCENARIOS related to Second Heart Sound (S2).
They are written in clinical vignette style exactly as used in AIIMS, NEET-PG, INI-CET, USMLE, PLAB level exams.
SECOND HEART SOUND (S2) – ALL POSSIBLE HARD CASE SCENARIOS
1. Fixed Wide Split S2
Scenario:
A 19-year-old female with recurrent respiratory infections and exertional dyspnea has a systolic ejection murmur at the pulmonary area. S2 splitting remains unchanged during inspiration and expiration.
Diagnosis: Atrial Septal Defect (Ostium secundum)
Key Mechanism: Constant RV volume overload → constant delayed P2
2. Paradoxical (Reversed) Splitting
Scenario:
A 68-year-old man with ischemic cardiomyopathy has S2 split heard during expiration that disappears on inspiration.
Diagnosis: Left bundle branch block / Severe aortic stenosis
Mechanism: Delayed A2 due to delayed LV depolarization or prolonged LV ejection
3. Wide Physiological Splitting
Scenario:
A young adult with a systolic murmur, normal respiration-dependent widening of S2, louder on inspiration.
Diagnosis: Pulmonary stenosis / RBBB
Mechanism: Prolonged RV systole → delayed P2
4. Single S2 – Severe Aortic Stenosis
Scenario:
A 72-year-old man with syncope, angina, and dyspnea has a harsh ejection systolic murmur radiating to carotids. S2 is single.
Cause: Absent or inaudible A2 due to calcified immobile aortic valve
5. Single S2 – Severe Pulmonary Stenosis
Scenario:
A cyanotic child with exertional fatigue has soft or absent P2.
Cause: Reduced pulmonary valve mobility
6. Loud A2
Scenario:
A patient with long-standing uncontrolled hypertension has a loud metallic S2 at right 2nd intercostal space.
Diagnosis: Systemic hypertension
Mechanism: High aortic pressure → forceful valve closure
7. Loud P2 (Accentuated P2)
Scenario:
A middle-aged woman with progressive dyspnea, raised JVP, and parasternal heave has a loud P2.
Diagnosis: Pulmonary arterial hypertension
Exam Pearl: Loud P2 = early sign of pulmonary HTN
8. Palpable P2
Scenario:
A patient with scleroderma presents with exertional dyspnea; P2 is palpable.
Diagnosis: Severe pulmonary hypertension
9. Soft or Absent A2
Scenario:
An elderly patient with collapsing pulse and early diastolic murmur has a faint A2.
Diagnosis: Severe aortic regurgitation
Mechanism: Rapid pressure equalization → ineffective valve closure
10. Soft P2
Scenario:
A patient with congenital heart disease has diminished P2 intensity.
Diagnosis: Pulmonary stenosis
11. Acute Pulmonary Embolism
Scenario:
Sudden dyspnea, chest pain, tachycardia, and new wide splitting of S2.
Mechanism: Acute RV strain → delayed P2
12. Mitral Stenosis Progression
Scenario:
A patient with long-standing rheumatic MS develops loud P2.
Implication: Development of pulmonary hypertension
13. ASD vs Pulmonary Stenosis Differentiation
Scenario:
Wide split S2 heard; does not change with respiration.
Answer: ASD (not PS)
Key Differentiator: Fixed splitting
14. LBBB vs RBBB
Scenario:
S2 split disappears during inspiration.
Diagnosis: LBBB
Contrast:
RBBB → delayed P2 → wide split on inspiration
15. Eisenmenger Syndrome
Scenario:
Adult with cyanosis, loud single S2, and pulmonary hypertension.
Cause: Loud P2 with loss of A2 component
16. Heart Failure with Reduced Ejection Fraction
Scenario:
Delayed A2 due to prolonged LV ejection → paradoxical split S2.
17. Hypertrophic Obstructive Cardiomyopathy
Scenario:
Young patient with syncope and paradoxical S2 splitting.
Mechanism: Prolonged LV ejection
18. Post-Valve Replacement
Scenario:
Mechanical valve patient with loud clicking A2.
Cause: Prosthetic valve closure sound
19. Normal Young Adult
Scenario:
Split S2 only during inspiration, disappears in expiration.
Diagnosis: Normal physiological splitting
20. Severe Pulmonary Hypertension with RV Failure
Scenario:
Single loud S2, dominant P2, signs of right heart failure.
Mechanism: A2 becomes inaudible due to dominance of P2
ULTIMATE EXAM PEARLS
- Fixed split = ASD
- Loud P2 = Pulmonary HTN
- Soft/absent A2 = Severe AS or AR
- Paradoxical split = LBBB or Severe AS
- Single S2 = Severe semilunar valve disease
If you want next (just say):
- Ultra-hard MCQs from these scenarios
- Flowchart to identify S2 abnormalities
- Comparison table: S2 vs S3 vs S4
- Clinical OSCE viva answers
I will keep it exam-killer level.
You’re absolutely right 👍 — those are important, high-yield causes affecting S2, and they should be included.
Thank you for pointing it out. Below is a CAUSE-BASED, CLINICAL CASE SCENARIO explanation specifically covering each condition you mentioned, focused on how and why S2 is altered.
This is exam-level integration, not omission.
SECOND HEART SOUND (S2): MISSED BUT IMPORTANT CAUSE-BASED CASE SCENARIOS
1. Wet Beriberi (Thiamine Deficiency – High Output Failure)
Case Scenario
A malnourished alcoholic presents with tachycardia, bounding pulses, warm extremities, and signs of heart failure. On auscultation, S2 is loud.
S2 Finding
- Loud S2 (especially A2)
Mechanism
- High cardiac output
- Increased stroke volume
- Forceful semilunar valve closure
📌 Exam Pearl: High-output states → loud S2
2. Coxsackie B Virus Myocarditis
Case Scenario
A young adult presents with viral prodrome followed by chest pain and acute heart failure. ECG shows ST changes. S2 is soft.
S2 Finding
- Soft S2
- Possible single S2
Mechanism
- Depressed ventricular contractility
- Reduced force of valve closure
📌 Key Point: Myocardial weakness → reduced S2 intensity
3. Wolff–Parkinson–White (WPW) Syndrome
Case Scenario
Young patient with recurrent palpitations and syncope. Auscultation reveals variable S2 splitting.
S2 Finding
- Variable or abnormal splitting
Mechanism
- Abnormal ventricular activation
- Altered timing of ventricular systole
- Inconsistent A2–P2 relationship
📌 Exam Insight: Electrical conduction disorders → altered S2 timing
4. Bundle Branch Block (BBB)
A. Right Bundle Branch Block (RBBB)
Scenario:
ECG shows RBBB. S2 splitting widens on inspiration.
S2 Finding:
- Wide splitting
Mechanism:
Delayed RV depolarization → delayed P2
B. Left Bundle Branch Block (LBBB)
Scenario:
Elderly patient with cardiomyopathy. Split S2 heard only in expiration.
S2 Finding:
- Paradoxical splitting
Mechanism:
Delayed LV depolarization → delayed A2
5. Down Syndrome
Case Scenario
Child with Down syndrome has recurrent respiratory infections. Auscultation shows fixed wide split S2.
S2 Finding
- Fixed splitting
Cause
- Atrial septal defect
- Atrioventricular septal defect
Mechanism
Constant RV volume overload → fixed delayed P2
📌 Association to Remember:
Down syndrome → AV canal defect → fixed S2 split
6. Severe Anemia
Case Scenario
Young woman with Hb 4 g/dL, flow murmur, bounding pulse, loud heart sounds.
S2 Finding
- Loud S2
Mechanism
- High-output cardiac state
- Increased velocity of blood flow
- Forceful valve closure
📌 Rule: Severe anemia behaves like hyperdynamic circulation
7. Patent Ductus Arteriosus (PDA)
Case Scenario
Child with continuous machinery murmur and bounding pulse. S2 is loud.
S2 Finding
- Loud P2
Mechanism
- Increased pulmonary blood flow
- Pulmonary hypertension (late)
- Forceful pulmonary valve closure
📌 Late PDA: Loud P2 → pulmonary HTN
8. Anterior Wall Myocardial Infarction
Case Scenario
Middle-aged man with acute chest pain, ECG showing anterior wall MI. S2 is soft.
S2 Finding
- Soft A2
- May become single S2
Mechanism
- LV systolic dysfunction
- Reduced force of aortic valve closure
📌 MI + LV failure → soft S2
INTEGRATED EXAM TABLE (VERY HIGH YIELD)
| Condition | S2 Change | Mechanism |
| ----------------------- | ----------------- | ------------------------ |
| Wet beriberi | Loud S2 | High-output state |
| Severe anemia | Loud S2 | Hyperdynamic circulation |
| Coxsackie B myocarditis | Soft S2 | Weak contraction |
| WPW | Variable split | Abnormal activation |
| RBBB | Wide split | Delayed P2 |
| LBBB | Paradoxical split | Delayed A2 |
| Down syndrome | Fixed split | ASD/AV canal |
| PDA | Loud P2 | Pulmonary HTN |
| Anterior wall MI | Soft A2 | LV dysfunction |
ULTIMATE MEMORY RULE
> Anything that increases flow/pressure → loud S2
> Anything that weakens ventricle → soft S2
> Anything that delays conduction → abnormal splitting