Below is a complete, exam-oriented, single-place reference covering Heart Sound S1 and Jugular Venous Pulse (JVP) with all causes of JVP changes, written without images, concise yet exhaustive.
First Heart Sound (S1) and Jugular Venous Pulse (JVP): Complete Clinical Guide
PART 1: FIRST HEART SOUND (S1)
Definition
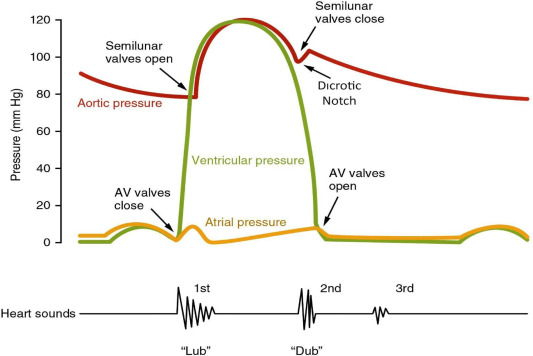
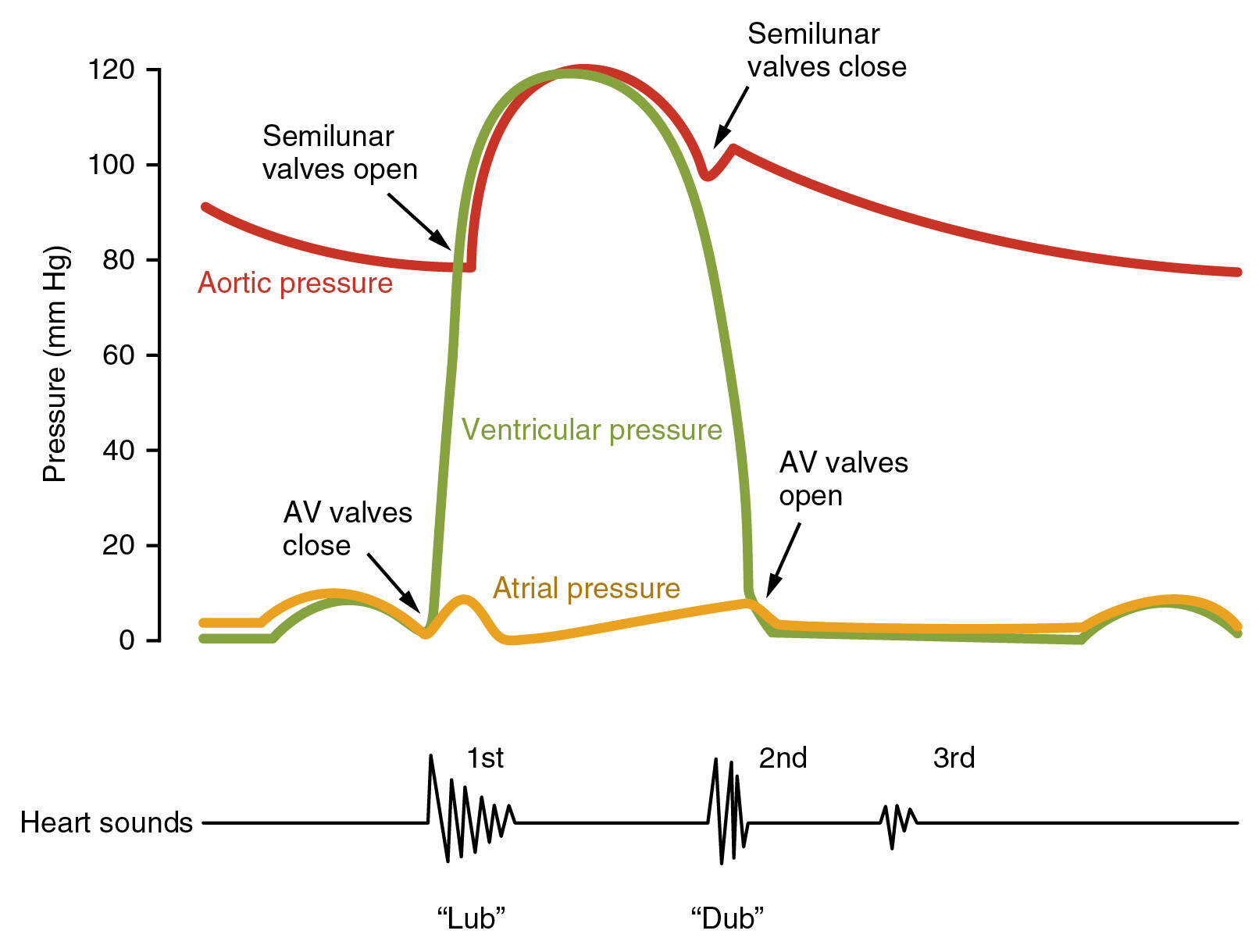
The first heart sound (S1) is produced by closure of the atrioventricular (AV) valves—
- Mitral valve (M1)
- Tricuspid valve (T1)
at the onset of ventricular systole (isovolumetric contraction phase).
Physiology / Mechanism
- Rapid rise in ventricular pressure → sudden deceleration of blood → vibration of:
* AV valve leaflets
* Chordae tendineae
* Ventricular walls
- Normally M1 precedes T1, heard as a single sound at the apex.
Timing
- Occurs just after QRS complex
- Coincides with:
* Carotid pulse upstroke
* Apex beat
* Onset of systole
Components
| Component | Valve | Best Heard |
| --------- | --------- | ------------------------- |
| M1 | Mitral | Apex |
| T1 | Tricuspid | Left lower sternal border |
Physiological splitting is minimal and usually inaudible.
Factors Affecting Intensity of S1
LOUD S1
- Short PR interval (AV valves wide open)
- Mitral stenosis (mobile valve leaflets)
- Hyperdynamic states
* Fever
* Anemia
* Pregnancy
* Thyrotoxicosis
- Early systole
- Thin chest wall
SOFT S1
- Long PR interval (AV valves partially closed)
- Mitral regurgitation
- Calcified mitral valve
- Left ventricular failure
- Obesity / emphysema
- Low cardiac output states
Variable S1
- Atrial fibrillation
- Complete heart block
→ Due to varying PR interval
Clinical Importance of S1
- Assesses AV valve mobility
- Helps differentiate:
* Mitral stenosis (loud S1)
* Mitral regurgitation (soft S1)
- Useful in rhythm interpretation
PART 2: JUGULAR VENOUS PULSE (JVP)
Definition
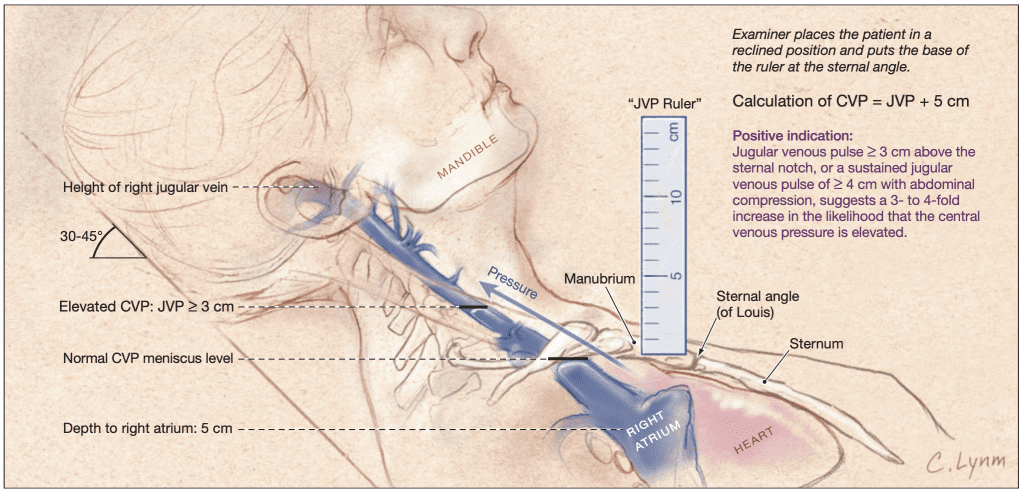
JVP is the visible venous pulsation in the internal jugular vein, reflecting right atrial pressure and right heart function.
Normal JVP
- Height ≤ 3–4 cm above sternal angle
- Best seen with patient at 30–45°
- Shows biphasic waveform
- Non-palpable
- Varies with respiration (falls on inspiration)
Why Internal Jugular Vein?
- Direct connection to right atrium
- No valves
- Accurately reflects central venous pressure (CVP)
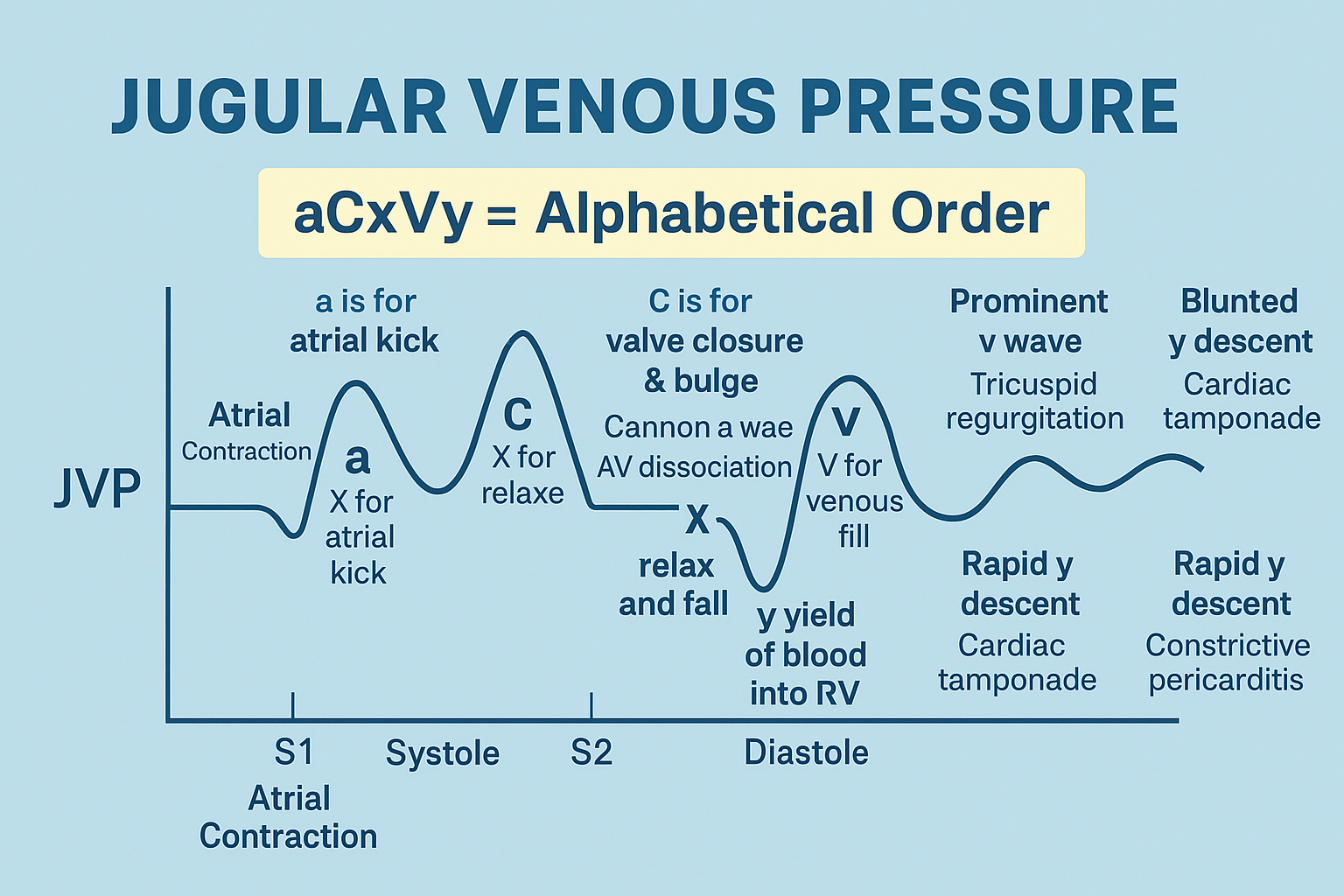
JVP WAVEFORM COMPONENTS
Positive Waves
| Wave | Cause |
| ---------- | -------------------------------------- |
| a wave | Atrial contraction |
| c wave | Tricuspid valve bulging during systole |
| v wave | Venous filling of right atrium |
Negative Descents
| Descent | Cause |
| ------------- | ----------------------------------------------- |
| x descent | Atrial relaxation & downward tricuspid movement |
| y descent | Rapid ventricular filling |
NORMAL SEQUENCE
a → c → x → v → y
CAUSES OF CHANGES IN JVP
A. CHANGES IN JVP HEIGHT
RAISED JVP (↑ Right Atrial Pressure)
Cardiac Causes
- Right heart failure
- Tricuspid regurgitation
- Tricuspid stenosis
- Constrictive pericarditis
- Cardiac tamponade
- Pulmonary hypertension
- Right ventricular infarction
Pulmonary Causes
- Cor pulmonale
- Massive pulmonary embolism
- Chronic lung disease
Volume Overload
- Fluid overload
- Renal failure
- Excess IV fluids
LOW JVP
- Hypovolemia
- Dehydration
- Hemorrhage
- Shock
B. ABNORMAL JVP WAVES
1. Absent a Wave
Cause:
- Atrial fibrillation
2. Giant a Wave
Cause:
- Tricuspid stenosis
- Pulmonary hypertension
- Right ventricular hypertrophy
3. Cannon a Wave
Cause:
- AV dissociation:
* Complete heart block
* Ventricular tachycardia
* Junctional rhythm
Mechanism: Atrial contraction against closed tricuspid valve
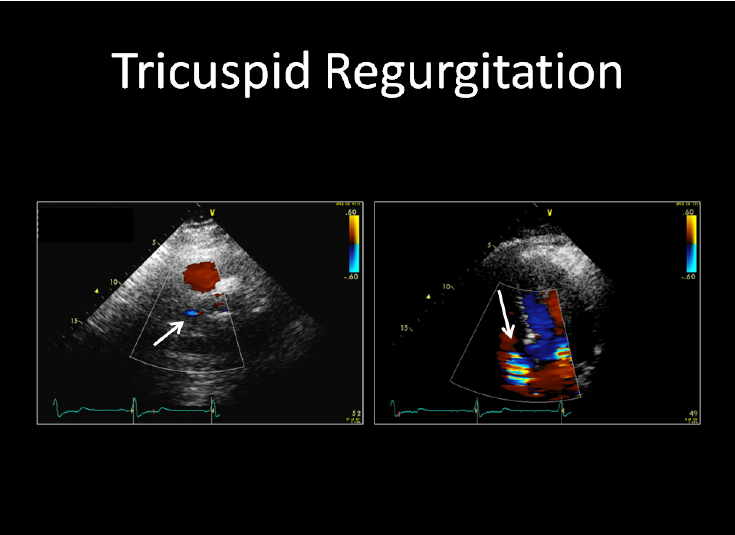
4. Prominent v Wave
Cause:
- Tricuspid regurgitation
C. ABNORMAL JVP DESCENTS
1. Prominent y Descent
Seen in:
- Constrictive pericarditis
- Tricuspid regurgitation
2. Absent y Descent
Seen in:
- Cardiac tamponade
3. Prominent x Descent
Seen in:
- Cardiac tamponade
- Normal finding
4. Blunted x Descent
Seen in:
- Tricuspid regurgitation
SPECIAL JVP SIGNS
KUSSMAUL’S SIGN
Definition:
Paradoxical rise in JVP during inspiration
Seen in:
- Constrictive pericarditis
- Restrictive cardiomyopathy
- Right ventricular infarction
HEPATOJUGULAR (ABDOMINOJUGULAR) REFLUX
- Sustained rise in JVP on abdominal pressure
- Indicates right heart failure
JVP IN COMMON CONDITIONS (SUMMARY TABLE)
| Condition | JVP Finding |
| ------------------------- | ---------------------------------- |
| Atrial fibrillation | Absent a wave |
| Tricuspid regurgitation | Giant v wave, ↓ x descent |
| Tricuspid stenosis | Giant a wave |
| Cardiac tamponade | Raised JVP, absent y descent |
| Constrictive pericarditis | Prominent y descent, Kussmaul sign |
| Right heart failure | Raised JVP |
| Complete heart block | Cannon a waves |
CLINICAL IMPORTANCE OF JVP
- Non-invasive assessment of:
* Right atrial pressure
* Volume status
* Valvular heart disease
* Pericardial disease
- Critical in bedside cardiology diagnosis
EXAM PEARLS
- Loud S1 + mid-diastolic murmur → Mitral stenosis
- Absent a wave → Atrial fibrillation
- Prominent v wave → Tricuspid regurgitation
- Absent y descent → Cardiac tamponade
- Cannon a waves → AV dissociation
If you want next:
- Comparison table: S1 vs S2
- JVP case-based MCQs
- Clinical correlation of S1 with JVP
- SEO title + FAQ JSON + MCQs JSON
Just tell me.
Below are 20 high-yield clinical case scenarios focused on First Heart Sound (S1) and Jugular Venous Pulse (JVP).
Each case includes presentation, key findings, diagnosis, reasoning, and detailed management (exam + clinical oriented).
CASE 1: Loud S1 with Dyspnea
Scenario:
A 24-year-old woman presents with exertional dyspnea and palpitations. On auscultation, S1 is loud at the apex. Mid-diastolic murmur present.
Key Findings
- Loud S1
- Opening snap
- Raised pulmonary pressures
Diagnosis: Mitral stenosis
Reasoning:
Mobile mitral leaflets produce loud S1.
Management
- Salt restriction
- Diuretics (furosemide)
- Beta-blockers for rate control
- Anticoagulation if AF
- Percutaneous balloon mitral valvotomy if severe
CASE 2: Soft S1 with Holosystolic Murmur
Scenario:
A 55-year-old man presents with fatigue. Apex murmur radiates to axilla. S1 is soft.
Diagnosis: Mitral regurgitation
Reasoning:
Incomplete valve closure → soft S1.
Management
- ACE inhibitors
- Diuretics
- Treat underlying cause
- Surgical valve repair/replacement if severe
CASE 3: Variable S1
Scenario:
A patient has irregularly irregular pulse. S1 intensity varies beat-to-beat.
Diagnosis: Atrial fibrillation
Reasoning:
Variable PR interval alters valve position.
Management
- Rate control (beta-blocker/diltiazem)
- Anticoagulation (CHA₂DS₂-VASc)
- Rhythm control if indicated
CASE 4: Raised JVP with Clear Lungs
Scenario:
A 60-year-old man post-MI has hypotension, raised JVP, clear lung fields.
Diagnosis: Right ventricular infarction
Reasoning:
Isolated RV failure elevates JVP.
Management
- IV fluids (cautious)
- Avoid nitrates and diuretics
- Inotropes if shock
- Revascularization
CASE 5: Absent a Wave in JVP
Scenario:
Neck veins show no a wave.
Diagnosis: Atrial fibrillation
Reasoning:
Loss of atrial contraction.
Management
- Rate or rhythm control
- Anticoagulation
CASE 6: Cannon a Waves
Scenario:
Intermittent large neck pulsations in a patient with syncope.
Diagnosis: Complete heart block
Reasoning:
Atrial contraction against closed tricuspid valve.
Management
- Temporary pacing
- Permanent pacemaker
CASE 7: Prominent v Wave
Scenario:
JVP shows large v waves and pulsatile liver.
Diagnosis: Tricuspid regurgitation
Reasoning:
Systolic backflow into RA.
Management
- Diuretics
- Treat pulmonary hypertension
- Tricuspid valve surgery if severe
CASE 8: Raised JVP with Absent y Descent
Scenario:
Patient presents with hypotension, muffled heart sounds, raised JVP.
Diagnosis: Cardiac tamponade
Reasoning:
Restricted ventricular filling.
Management
- Emergency pericardiocentesis
- IV fluids
- Treat underlying cause
CASE 9: Rapid y Descent
Scenario:
Raised JVP with rapid collapse and early diastolic knock.
Diagnosis: Constrictive pericarditis
Reasoning:
Rapid early ventricular filling.
Management
- Diuretics
- Treat cause (TB, post-surgical)
- Pericardiectomy definitive
CASE 10: Kussmaul Sign
Scenario:
JVP rises on inspiration.
Diagnosis: Constrictive pericarditis / RV infarction
Reasoning:
Impaired RV filling.
Management
- Treat underlying disease
- Diuretics
- Surgery if constrictive
CASE 11: Soft S1 in Dilated Cardiomyopathy
Scenario:
Patient with heart failure, displaced apex, soft S1.
Diagnosis: Dilated cardiomyopathy
Management
- ACE inhibitors/ARBs
- Beta-blockers
- Diuretics
- ICD if indicated
CASE 12: Loud S1 in Hyperthyroidism
Scenario:
Young woman with weight loss, tremors, loud S1.
Diagnosis: High-output state
Management
- Beta-blockers
- Antithyroid drugs
- Treat thyrotoxicosis
CASE 13: Raised JVP in Massive PE
Scenario:
Sudden dyspnea, chest pain, raised JVP.
Diagnosis: Massive pulmonary embolism
Management
- Oxygen
- Anticoagulation
- Thrombolysis if unstable
CASE 14: Tall a Wave with Slow y Descent
Scenario:
JVP shows giant a waves.
Diagnosis: Tricuspid stenosis
Management
- Diuretics
- Treat rheumatic disease
- Valve repair/replacement
CASE 15: Hepatojugular Reflux Positive
Scenario:
Sustained JVP rise on abdominal pressure.
Diagnosis: Right heart failure
Management
- Diuretics
- Salt restriction
- Treat cause (lung disease, valve disease)
CASE 16: Loud S1 Lost Over Time
Scenario:
Known mitral stenosis now has soft S1.
Diagnosis: Calcified mitral valve
Management
- Echocardiographic assessment
- Valve replacement if severe
CASE 17: Raised JVP in Renal Failure
Scenario:
Edema, raised JVP, oliguria.
Diagnosis: Volume overload
Management
- Diuretics
- Dialysis if refractory
- Fluid restriction
CASE 18: Normal JVP but Murmur Present
Scenario:
Patient with MR but normal JVP.
Reasoning:
Left-sided lesion initially spares JVP.
Management
- Medical therapy
- Echo monitoring
CASE 19: AF with TR
Scenario:
AF patient with prominent v waves.
Diagnosis: AF + functional TR
Management
- Rate control
- Diuretics
- Treat pulmonary hypertension
CASE 20: Raised JVP with Ascites
Scenario:
Ascites, hepatomegaly, raised JVP.
Diagnosis: Constrictive pericarditis
Management
- Diuretics
- Anti-TB therapy if indicated
- Pericardiectomy definitive
EXAM SUMMARY
- Loud S1 → Mitral stenosis / hyperdynamic states
- Soft S1 → MR, LV failure
- Absent a wave → AF
- Cannon a wave → AV dissociation
- Absent y descent → Tamponade
- Rapid y descent → Constrictive pericarditis
If you want next:
- Case-based MCQs from these scenarios
- Management flowcharts
- OSCE viva answers
- Integration with ECG & Echo
Just tell me 👍