First Heart Sound (S1) and Jugular Venous Pressure (JVP) – Complete Clinical Guide
PART A: FIRST HEART SOUND (S1)
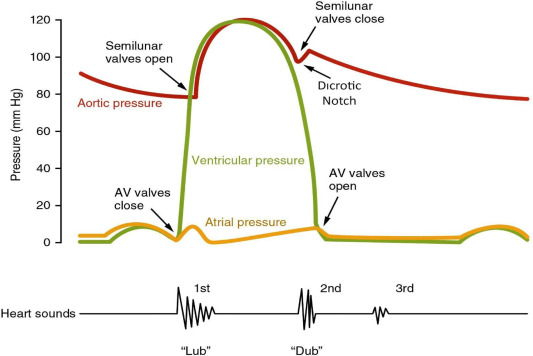
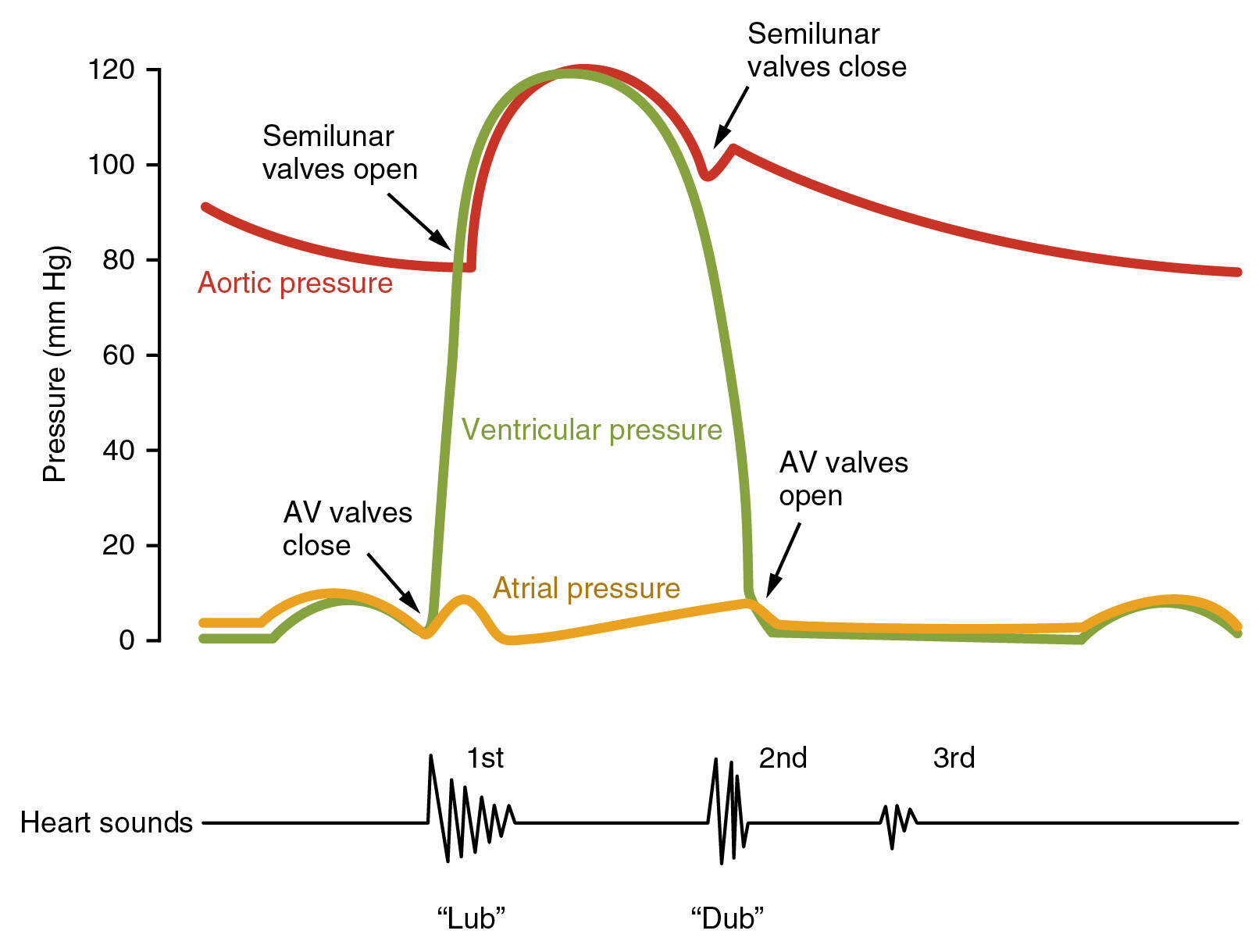
1. Definition
S1 is the first audible heart sound, produced mainly by closure of the atrioventricular valves (mitral and tricuspid) at the onset of ventricular systole.
2. Components of S1
- M1 (Mitral component) – louder, occurs slightly earlier
- T1 (Tricuspid component) – softer, slightly delayed
Normally heard as a single sound because the interval is very short.
3. Mechanism of Production
S1 results from:
- Sudden tensing of AV valve leaflets
- Vibration of:
* Valve apparatus
* Ventricular myocardium
* Blood column
Valve closure is not the sole cause; myocardial contraction plays a major role.
Reference:
https://www.ncbi.nlm.nih.gov/books/NBK333/
4. Timing and Auscultation
- Coincides with:
* Carotid pulse upstroke
* R wave of ECG
- Best heard at:
* Apex (mitral area)
* Lower left sternal border (tricuspid area)
5. Normal Characteristics of S1
- Low-pitched
- Longer duration than S2
- Best heard with bell of stethoscope
6. Variations in Intensity of S1
A. Loud S1
Causes:
- Mitral stenosis (mobile valve)
- Short PR interval (e.g., WPW)
- Tachycardia
- Hyperdynamic states (fever, anemia, thyrotoxicosis)
Mechanism: Valve leaflets wide open at onset of systole
B. Soft S1
Causes:
- Mitral regurgitation
- Long PR interval (first-degree AV block)
- Left ventricular dysfunction
- Calcified mitral valve
Mechanism: Valve partially closed before systole
C. Variable S1
Seen in:
- Atrial fibrillation
- Complete heart block
7. Split S1
Physiological Split
- Rarely audible
- Due to slight delay between M1 and T1
Wide Split
Seen in:
- Right bundle branch block
- Ebstein anomaly
8. Clinical Importance of S1
- Loud S1 → suggests mobile mitral valve
- Soft S1 → suggests poor ventricular contraction or MR
- Changing S1 → suggests arrhythmia
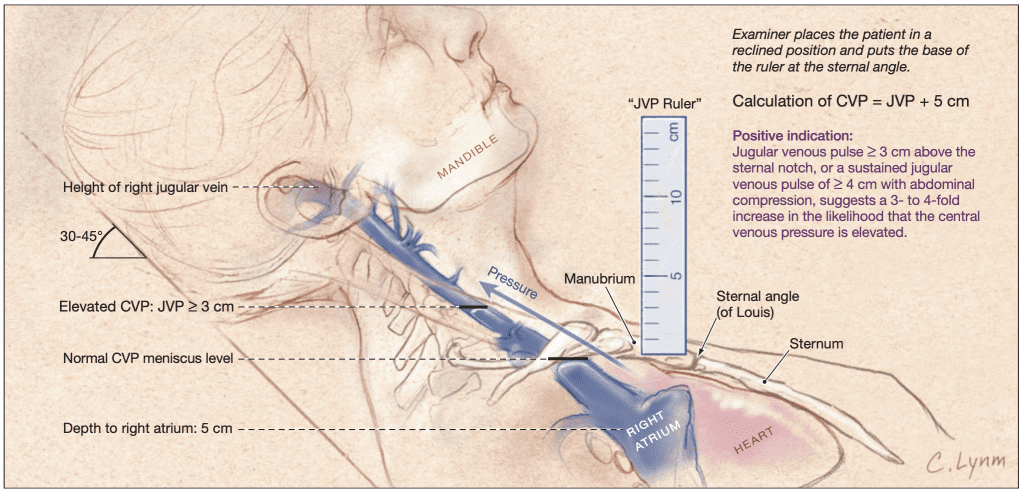
PART B: JUGULAR VENOUS PRESSURE (JVP)
1. Definition
JVP is an indirect clinical measurement of right atrial pressure, assessed by observing the internal jugular vein pulsations.
2. Why Internal Jugular Vein?
- Direct connection to right atrium
- No valves between vein and atrium
- Reflects central venous pressure accurately
3. Normal JVP
- ≤ 3–4 cm above sternal angle
(≈ 8–9 cm H₂O from right atrium)
4. Method of Examination
- Patient reclining at 30–45°
- Head turned slightly to the left
- Observe right side of neck
- Use tangential lighting
Key reference:
https://geekymedics.com/jugular-venous-pressure-jvp-examination/
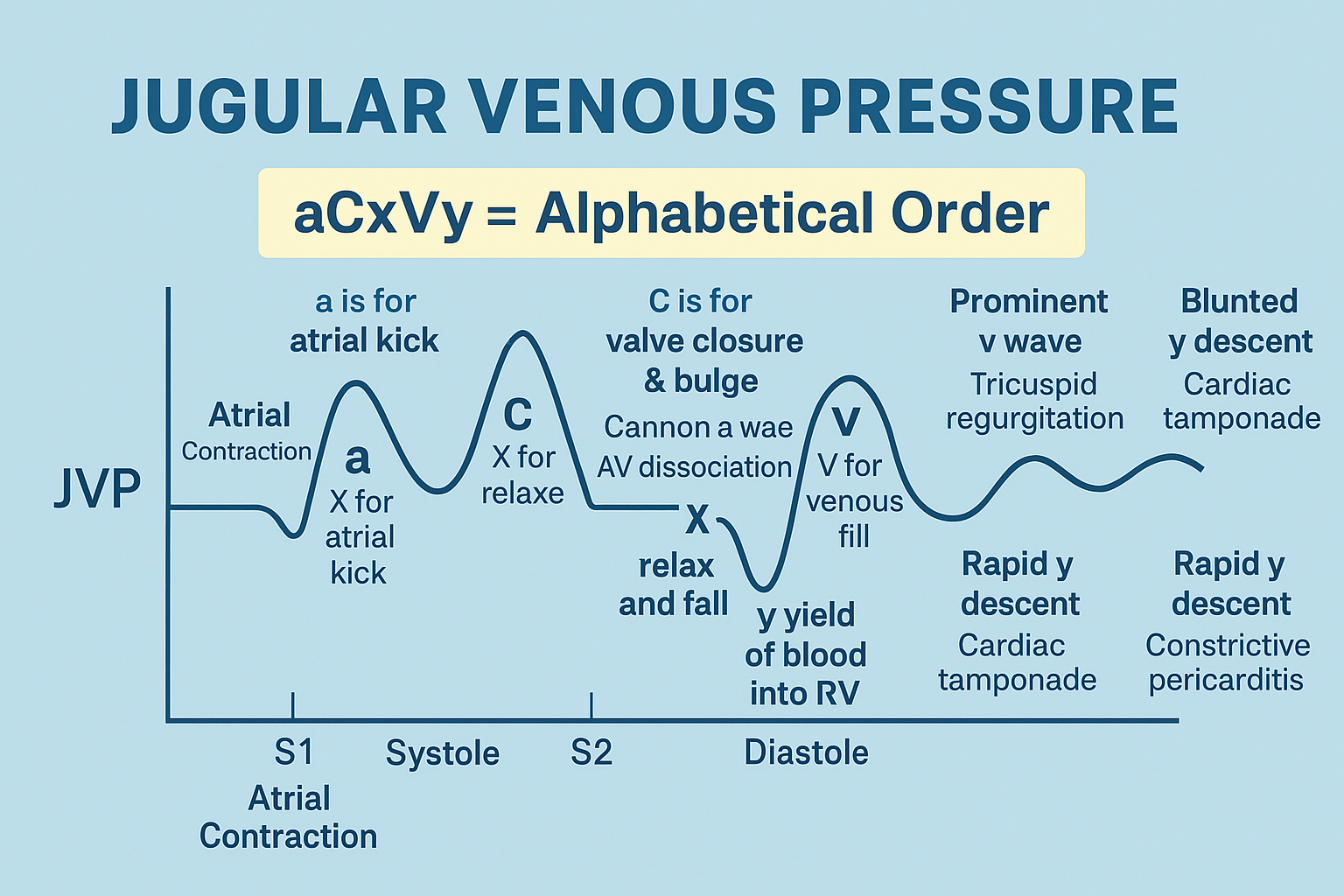
5. Normal JVP Waveform Components
A. a wave
- Atrial contraction
- Absent in atrial fibrillation
B. c wave
- Tricuspid valve bulging during early systole
- Often not visible clinically
C. x descent
- Atrial relaxation
- Downward displacement of tricuspid valve
D. v wave
- Venous filling against closed tricuspid valve
- Prominent in tricuspid regurgitation
E. y descent
- Rapid ventricular filling after tricuspid opening
6. Abnormal JVP Waveforms
A. Giant a wave
Causes:
- Tricuspid stenosis
- Pulmonary hypertension
- RV hypertrophy
B. Cannon a waves
Cause:
- AV dissociation
Seen in:
- Complete heart block
- Ventricular tachycardia
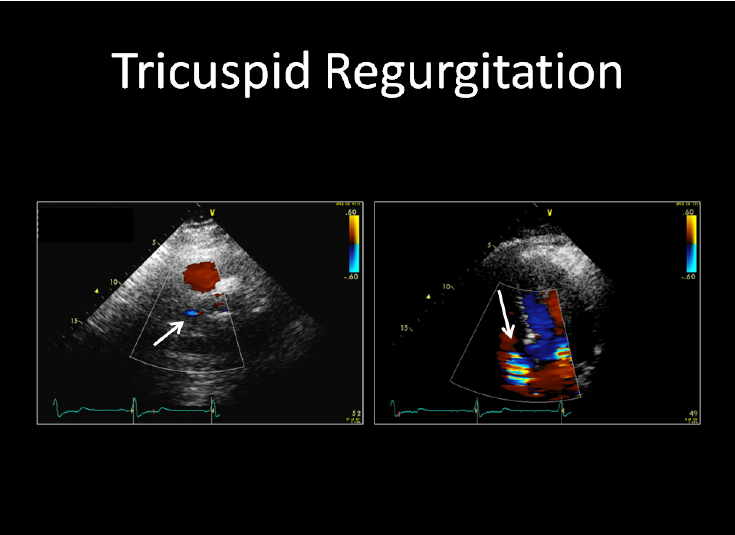
C. Prominent v wave
Cause:
- Tricuspid regurgitation
D. Absent a wave
Cause:
- Atrial fibrillation
7. Abnormal JVP Descents
A. Rapid y descent
Seen in:
- Constrictive pericarditis
- Tricuspid regurgitation
B. Slow y descent
Seen in:
- Tricuspid stenosis
C. Absent y descent
Seen in:
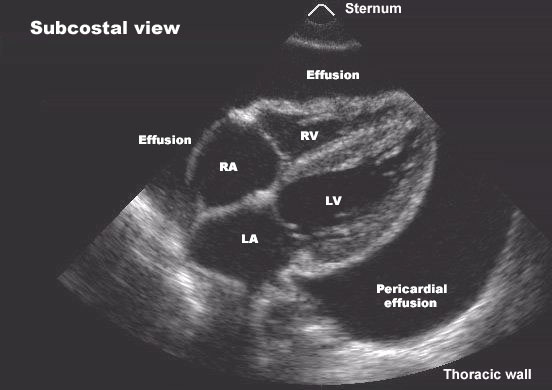
- Cardiac tamponade
8. Raised JVP – Causes
Cardiac Causes
- Right heart failure
- Tricuspid regurgitation
- Constrictive pericarditis
- Cardiac tamponade
Non-cardiac Causes
- Fluid overload
- Superior vena cava obstruction
9. Special JVP Signs
A. Kussmaul Sign
- Paradoxical rise in JVP during inspiration
Seen in:
- Constrictive pericarditis
- Restrictive cardiomyopathy
- RV infarction
B. Hepatojugular (Abdominojugular) Reflux
- Sustained rise in JVP with abdominal pressure
Indicates right heart failure
10. Differentiating JVP from Carotid Pulse
| Feature | JVP | Carotid |
| -------------------- | ----------- | ---------- |
| Palpable | No | Yes |
| Waveform | Biphasic | Monophasic |
| Changes with posture | Yes | No |
| Pressure effect | Obliterates | No |
11. Clinical Importance of JVP
- Bedside assessment of:
* Volume status
* Right heart function
- Helps diagnose:
* Heart failure
* Valvular disease
* Pericardial disease
12. Authoritative External References
- https://www.ncbi.nlm.nih.gov/books/NBK333/
- https://geekymedics.com/jugular-venous-pressure-jvp-examination/
- https://teachmephysiology.com/cardiovascular-system/heart-sounds/
- https://www.ahajournals.org
If you want next:
- Hard case-based MCQs (HTML/CSS/JS)
- FAQ JSON + MCQ JSON (exact exam format)
- Clinical case scenarios with management
- SEO-optimized title, description, and keywords
Just tell me 👍
Below are 25 high-yield, exam-oriented, detailed clinical case scenarios focused on First Heart Sound (S1) and Jugular Venous Pressure (JVP), each with interpretation and stepwise management.
(Structured for UG/PG exams, ward rounds, and viva.)
1. Loud S1 in Mitral Stenosis
Scenario:
A 26-year-old woman presents with exertional dyspnea and palpitations. Auscultation reveals a loud, tapping S1 with an opening snap.
Interpretation:
Mobile mitral valve leaflets in mitral stenosis → forceful closure → loud S1.
Management:
- Echocardiography to assess valve area
- Rate control (β-blockers)
- Anticoagulation if AF present
- Percutaneous balloon mitral valvotomy if suitable
2. Soft S1 in Mitral Regurgitation
Scenario:
A 52-year-old man has pansystolic murmur radiating to axilla and soft S1.
Interpretation:
Incomplete mitral valve closure before systole.
Management:
- Echo to quantify MR
- ACE inhibitors for LV unloading
- Surgical repair or replacement if severe
3. Variable S1 in Atrial Fibrillation
Scenario:
Irregularly irregular pulse with varying S1 intensity.
Interpretation:
Variable diastolic filling → variable AV valve position.
Management:
- Rate control (β-blocker, diltiazem)
- Anticoagulation (CHA₂DS₂-VASc guided)
- Rhythm control if indicated
4. Wide Split S1 in RBBB
Scenario:
Wide S1 split heard at left sternal border.
Interpretation:
Delayed tricuspid valve closure.
Management:
- ECG confirmation
- Treat underlying cause
- No specific therapy if asymptomatic
5. Loud S1 in Hyperthyroidism
Scenario:
Young woman with tremors, tachycardia, loud S1.
Interpretation:
Hyperdynamic circulation.
Management:
- β-blockers
- Antithyroid drugs
- Definitive therapy (radioiodine or surgery)
6. Soft S1 in Dilated Cardiomyopathy
Scenario:
Displaced apex, S3 present, soft S1.
Interpretation:
Poor ventricular contractility.
Management:
- ACE inhibitors / ARNI
- β-blockers
- Diuretics
- ICD if indicated
7. Giant a Waves in Pulmonary Hypertension
Scenario:
Raised JVP with prominent a waves.
Interpretation:
Forceful RA contraction against stiff RV.
Management:
- Treat cause of pulmonary hypertension
- Diuretics
- Pulmonary vasodilators
- Oxygen therapy
8. Cannon a Waves in Complete Heart Block
Scenario:
Intermittent large neck pulsations.
Interpretation:
Atrial contraction against closed tricuspid valve.
Management:
- Temporary pacing if unstable
- Permanent pacemaker
9. Absent a Waves in Atrial Fibrillation
Scenario:
Raised JVP without a waves.
Interpretation:
Loss of atrial contraction.
Management:
- Rate control
- Anticoagulation
- Rhythm control if suitable
10. Prominent v Waves in Tricuspid Regurgitation
Scenario:
Pulsatile neck veins with systolic expansion.
Interpretation:
Systolic backflow into RA.
Management:
- Diuretics
- Treat pulmonary hypertension
- Surgical repair if severe
11. Rapid y Descent in Constrictive Pericarditis
Scenario:
Raised JVP with sharp y descent.
Interpretation:
Rapid early filling with abrupt halt.
Management:
- Diuretics
- Pericardiectomy definitive
12. Absent y Descent in Cardiac Tamponade
Scenario:
Hypotension, muffled heart sounds, raised JVP.
Interpretation:
Restricted ventricular filling.
Management:
- Emergency pericardiocentesis
- Treat underlying cause
13. Kussmaul Sign in RV Infarction
Scenario:
JVP rises on inspiration after inferior MI.
Interpretation:
Impaired RV filling.
Management:
- Volume loading
- Avoid nitrates
- Revascularization
14. Positive Hepatojugular Reflux
Scenario:
Sustained JVP rise with abdominal pressure.
Interpretation:
Reduced RV reserve.
Management:
- Optimize heart failure therapy
- Diuretics
- Treat underlying cause
15. Low JVP in Hypovolemia
Scenario:
Collapsed neck veins, tachycardia.
Interpretation:
Low right atrial pressure.
Management:
- IV fluids
- Treat cause (bleeding, dehydration)
16. Loud S1 with Short PR Interval
Scenario:
Young patient with palpitations and loud S1.
Interpretation:
AV valves wide open at systole.
Management:
- ECG evaluation
- Treat pre-excitation if present
17. Soft S1 in First-Degree AV Block
Scenario:
PR interval 320 ms, soft S1.
Interpretation:
Partial AV valve closure before systole.
Management:
- Usually no treatment
- Review AV-nodal drugs
18. Raised JVP in Right Heart Failure
Scenario:
Peripheral edema, hepatomegaly, raised JVP.
Interpretation:
Elevated RA pressure.
Management:
- Diuretics
- Treat LV failure or pulmonary cause
19. JVP in Superior Vena Cava Obstruction
Scenario:
Raised JVP, facial swelling, non-pulsatile veins.
Interpretation:
Venous obstruction, not cardiac.
Management:
- Imaging (CT chest)
- Treat malignancy or thrombosis
20. Soft S1 in Calcified Mitral Valve
Scenario:
Elderly patient with MS but soft S1.
Interpretation:
Immobile calcified leaflets.
Management:
- Medical therapy
- Valve replacement if severe
21. Wide S1 Split in Ebstein Anomaly
Scenario:
Young adult with cyanosis and split S1.
Interpretation:
Delayed tricuspid closure.
Management:
- Echo confirmation
- Surgical correction if symptomatic
22. Raised JVP with Normal Heart Sounds
Scenario:
Raised JVP but normal S1 and S2.
Interpretation:
Fluid overload.
Management:
- Diuretics
- Fluid restriction
23. Prominent x Descent in Cardiac Tamponade
Scenario:
Sharp x descent, absent y descent.
Interpretation:
Preserved atrial relaxation.
Management:
- Emergency pericardial drainage
24. Loud S1 in Early Mitral Stenosis
Scenario:
Asymptomatic patient, loud S1 only.
Interpretation:
Early disease with mobile valve.
Management:
- Observation
- Secondary rheumatic fever prophylaxis
25. Combined Soft S1 and Raised JVP
Scenario:
Patient with cardiomyopathy and edema.
Interpretation:
Poor LV function + right heart failure.
Management:
- Guideline-directed heart failure therapy
- Device therapy if indicated