1. First Heart Sound (S1)
Definition
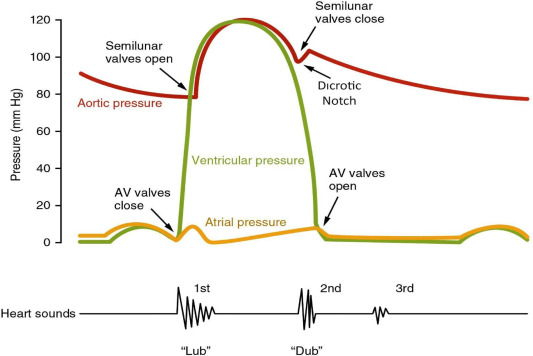
S1 is the sound produced by closure of atrioventricular (AV) valves—mitral (M1) followed by tricuspid (T1)—marking the onset of ventricular systole.
Mechanism
- Sudden deceleration of blood and vibration of valve leaflets, chordae, and ventricular walls
- Occurs at the end of ventricular filling when ventricular pressure exceeds atrial pressure
Normal Characteristics
- Best heard at apex
- Low-pitched, dull
- Coincides with carotid upstroke
- M1 slightly precedes T1 (physiological splitting)
Variations
Loud S1
- Mitral stenosis (mobile leaflets)
- Short PR interval
- Hyperdynamic states (thyrotoxicosis)
Soft S1
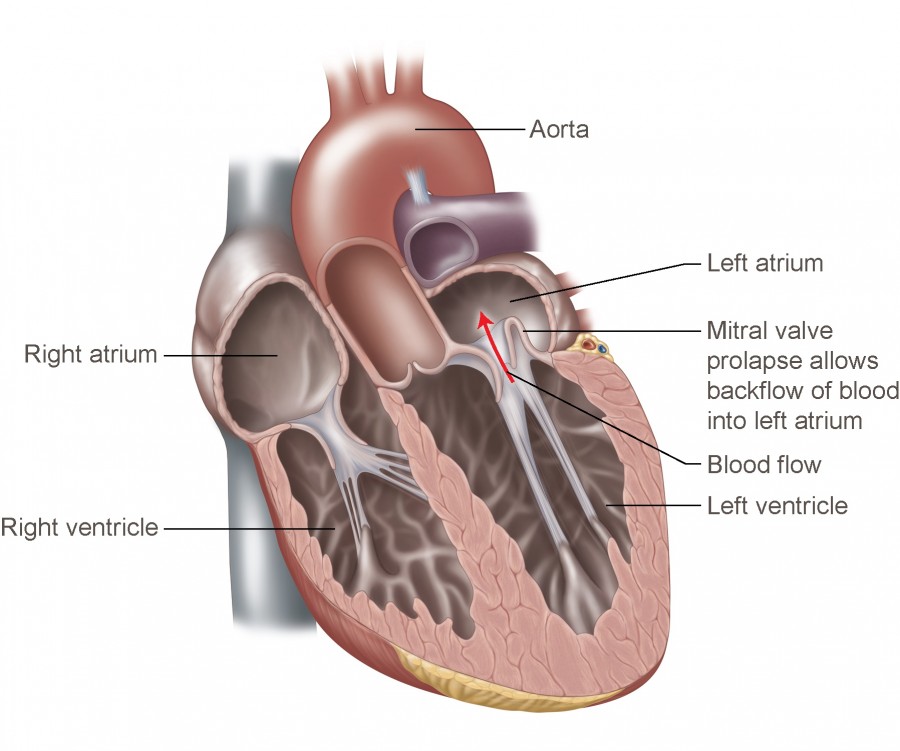
- Mitral regurgitation
- Long PR interval
- LV dysfunction
Variable S1
- Atrial fibrillation
- Complete heart block
Clinical Significance
- Reflects mitral valve mobility and ventricular contractility
- Loss of intensity suggests valvular damage or LV dysfunction
2. Third Heart Sound (S3)
Definition
A low-frequency sound occurring in early diastole, just after S2, during rapid ventricular filling.
Mechanism
- Sudden deceleration of blood entering a volume-overloaded ventricle
Physiological vs Pathological
Physiological
- Children, adolescents
- Pregnancy
- Athletes
Pathological (Adults >40 years)
- Dilated cardiomyopathy
- Congestive heart failure
- Mitral regurgitation
- Ventricular septal defect
Auscultation
- Best heard with bell at apex (LV S3)
- Left lateral position
Clinical Importance
- Indicates raised filling pressures
- Strong predictor of poor prognosis in heart failure
3. Fourth Heart Sound (S4)
Definition
A late diastolic sound caused by atrial contraction against a stiff ventricle.
Mechanism
- Atrial systole forces blood into non-compliant ventricle
Causes
- Hypertensive heart disease
- Aortic stenosis
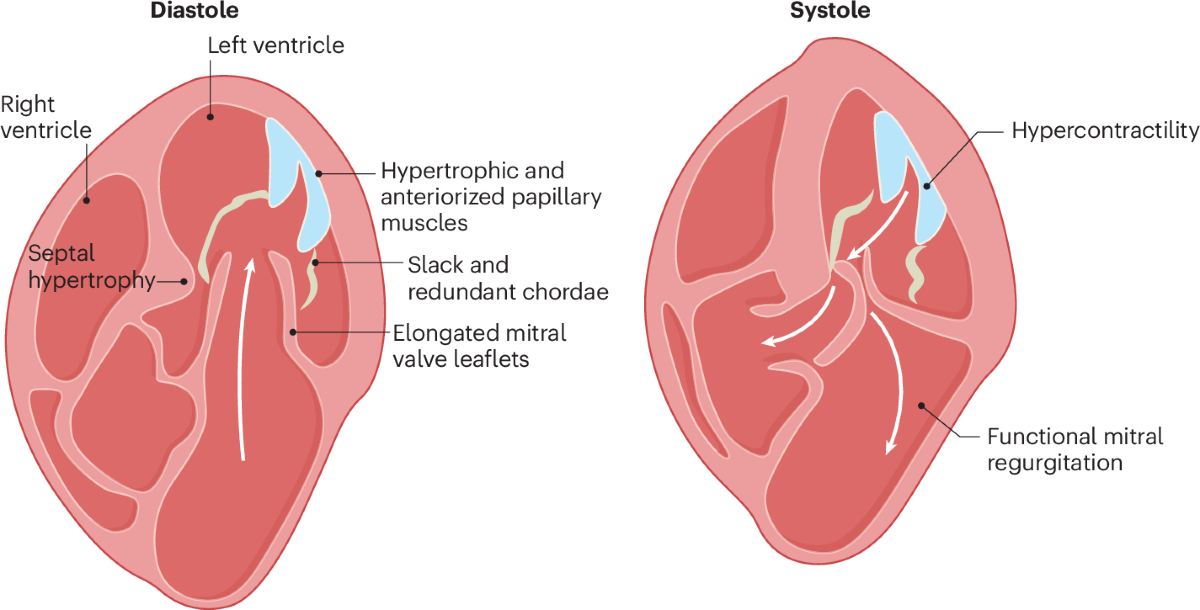
- Hypertrophic cardiomyopathy
- Ischemic heart disease
Key Features
- Occurs just before S1
- Best heard at apex
- Requires sinus rhythm
❌ Absent in atrial fibrillation
Clinical Significance
- Marker of diastolic dysfunction
- Often precedes overt heart failure
4. Atrial Myxoma
Definition
The most common primary cardiac tumor, usually benign, arising from interatrial septum (fossa ovalis).
Epidemiology
- Adults (30–60 years)
- Female predominance
- Mostly left atrium
Pathophysiology
- Pedunculated mass → ball-valve obstruction
- Can embolize or cause cytokine-mediated symptoms
Clinical Features (Classic Triad)
- Obstructive: Dyspnea, syncope, positional symptoms
- Embolic: Stroke, peripheral emboli
- Constitutional: Fever, weight loss (IL-6 mediated)
Physical Signs
- Early diastolic “tumor plop”
- Mimics mitral stenosis
- Changing murmur with posture
Diagnosis
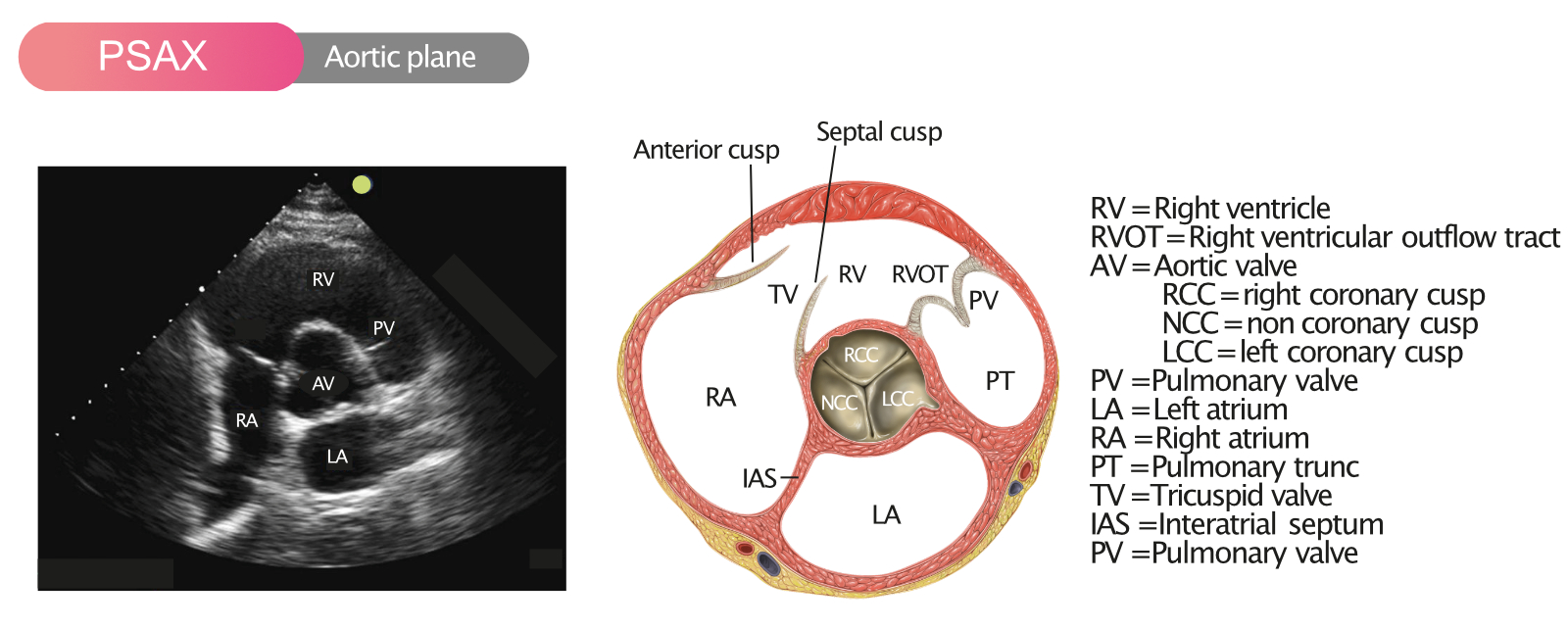
- Echocardiography (TTE / TEE)
- MRI for tissue characterization
Treatment
- Urgent surgical excision
Prognosis
- Excellent after removal
- Recurrence rare (familial forms higher)
5. Papillary Fibroelastoma
Definition
A benign avascular cardiac tumor arising from endocardial surfaces, most commonly cardiac valves.
Epidemiology
- Second most common primary cardiac tumor
- Common on aortic and mitral valves
Morphology
- Small, mobile
- “Sea-anemone” appearance
- Highly emboligenic despite small size
Clinical Manifestations
- Often asymptomatic
- Stroke, TIA
- MI (coronary embolism)
- Sudden death (rare)
Diagnosis
- Transesophageal echocardiography (gold standard)
Management
- Surgical excision if:
* Symptomatic
* Mobile
* Left-sided lesion
Prognosis
- Excellent post-excision
6. Tuberculous Pericarditis
Definition
Pericardial infection caused by Mycobacterium tuberculosis, common in endemic regions.
Pathogenesis
TB spread via:
- Lymphatics
- Hematogenous
- Direct extension from lungs
Stages
- Dry (fibrinous)
- Effusive
- Absorptive
- Constrictive
Clinical Features
- Fever, night sweats
- Chest pain
- Dyspnea
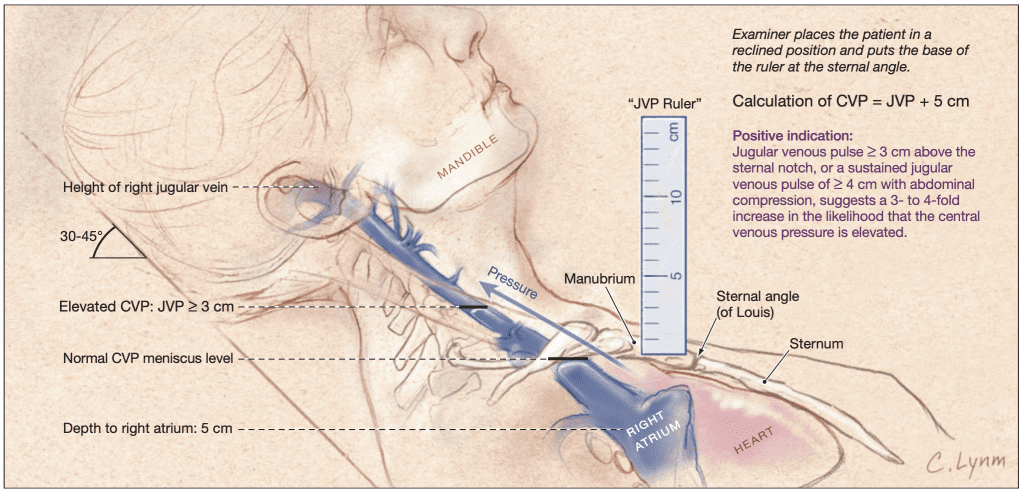
- Raised JVP
- Pulsus paradoxus (if tamponade)
Investigations
- Pericardial fluid:
* Exudative, lymphocytic
* ↑ ADA
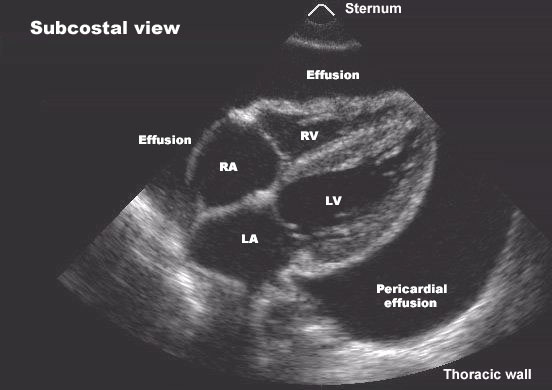
- Echocardiography
- CT/MRI
- Pericardial biopsy (definitive)
Treatment
Anti-tubercular therapy (ATT)
- Isoniazid
- Rifampicin
- Pyrazinamide
- Ethambutol
Adjunctive Corticosteroids
- Reduce inflammation
- Decrease risk of constriction
7. Complication After Treatment: Constrictive Pericarditis
Definition
A condition where thickened, fibrotic, sometimes calcified pericardium restricts diastolic filling.
Etiology
- Post-tuberculous pericarditis (commonest worldwide)
- Post-surgical
- Radiation
Pathophysiology
- Loss of pericardial elasticity
- Ventricular interdependence
- Equalization of diastolic pressures
Clinical Features
- Right-sided heart failure:
* Ascites
* Peripheral edema
* Hepatomegaly
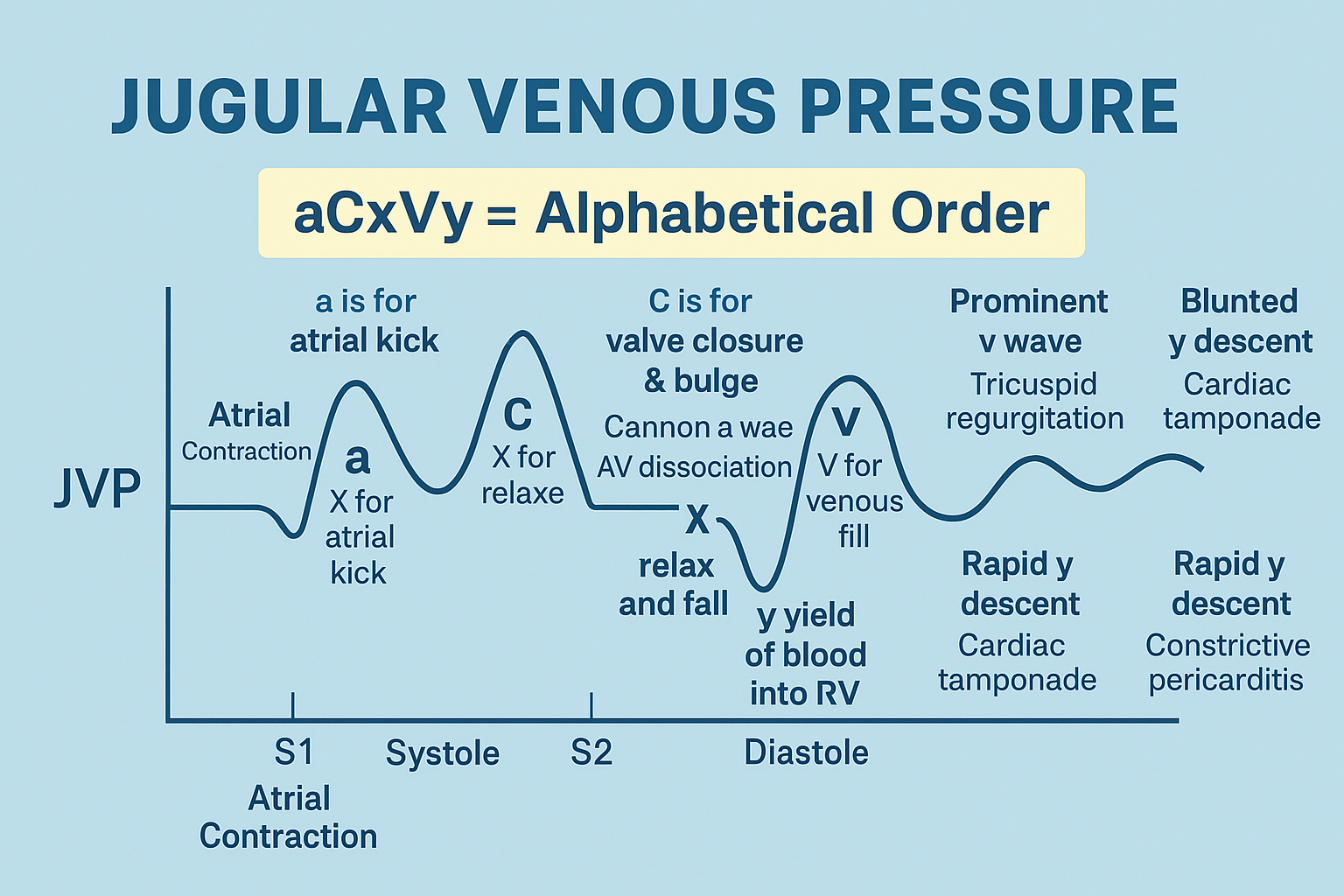
- Raised JVP with prominent y descent
- Kussmaul sign
- Pericardial knock (early diastole)
Investigations
- Echocardiography
- CT/MRI: pericardial thickening
- Cardiac catheterization (pressure equalization)
Management
- Diuretics (temporary)
- Definitive: Pericardiectomy
Prognosis
- Good if treated early
- Delayed diagnosis → irreversible myocardial atrophy
High-Yield Exam Correlations
- S3 = volume overload
- S4 = stiff ventricle
- Tumor plop = atrial myxoma
- TB pericarditis → constrictive pericarditis
- Pericardial knock ≠ S3