Ischemic Heart Disease — concise, complete reference
1) Definition & epidemiology
Ischemic heart disease (IHD), also called coronary artery disease (CAD) or coronary heart disease, is the set of clinical syndromes caused by an imbalance between myocardial oxygen supply and demand, most commonly from atherosclerotic narrowing or thrombosis of coronary arteries. Manifestations range from stable angina and silent ischemia to acute coronary syndromes (unstable angina, NSTEMI, STEMI) and ischemic cardiomyopathy. ([NCBI][1])
Global burden: IHD is the leading single cause of death worldwide and remains a major cause of disability; prevention and timely reperfusion/secondary prevention have reduced acute-mortality in well-resourced settings but chronic ASCVD burden remains high. (WHO, guideline summaries). ([World Health Organization][2])
2) Pathophysiology (short)
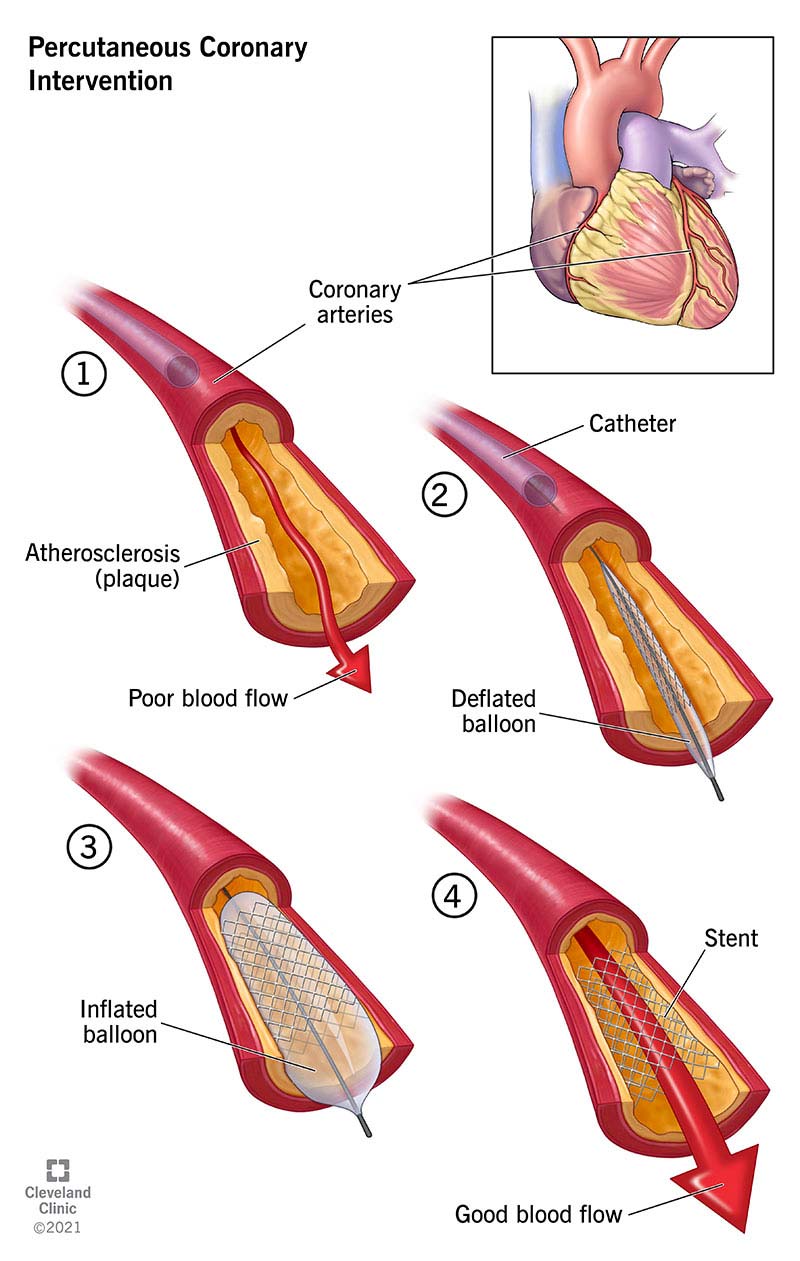
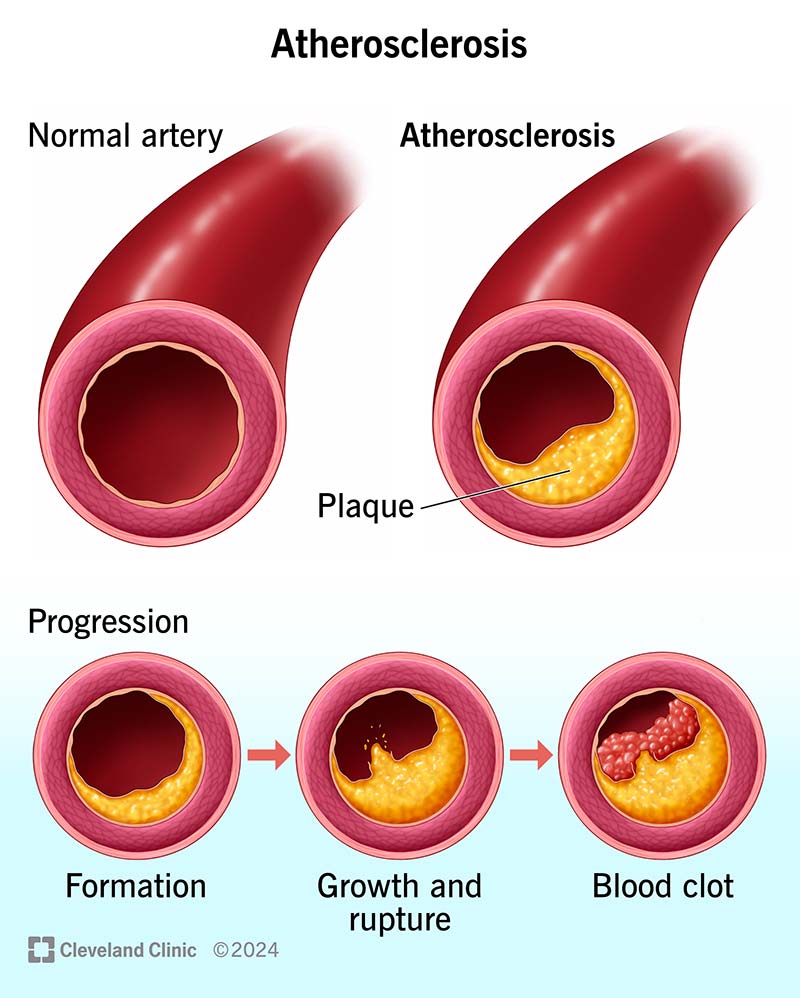
- Atherosclerotic plaque formation in epicardial coronary arteries → luminal narrowing and impaired flow reserve.
- Plaque rupture/erosion with superimposed thrombosis → abrupt coronary occlusion → myocardial ischemia/infarction (ACS).
- Microvascular dysfunction, coronary spasm, anemia, hypotension, tachyarrhythmia, or supply/demand mismatch can also produce ischemia without obstructive epicardial CAD. ([NCBI][1])
3) Causes / risk factors
Major modifiable: smoking, diabetes mellitus, hypertension, dyslipidaemia (↑LDL), obesity, physical inactivity, unhealthy diet.
Non-modifiable: age, male sex (though women catch up after menopause), family history/genetic predisposition.
Other contributors: chronic kidney disease, inflammatory diseases, HIV, cocaine/amphetamine use. ([World Health Organization][2])
4) Clinical features
- Stable angina: exertional chest discomfort (pressure/tightness), predictable, relieved by rest or nitrates.
- Unstable angina / NSTEMI: chest pain at rest, increasing frequency; biomarkers may be normal (UA) or elevated (NSTEMI).
- STEMI: prolonged chest pain with ST-segment elevation on ECG and biomarkers consistent with myocardial necrosis.
- Other presentations: dyspnea, syncope, atypical pain (especially in elderly, women, diabetics — may be “silent ischemia”). ([www.heart.org][3])
5) Investigations & diagnosis — practical approach
Immediate tests for suspected ACS:
- 12-lead ECG within 10 minutes (look for ST elevation, new LBBB, ST depression/ischemic changes).
- High-sensitivity troponin (serial: at presentation and 1–3 h or as per local protocol) to detect myocardial necrosis.
- Chest X-ray if needed for alternative diagnoses.
- Bedside vitals, IV access, oxygen only if hypoxaemic, continuous monitoring.
Further tests for stable disease or post-acute evaluation:
- Exercise ECG, stress imaging (stress echo, nuclear perfusion, stress CMR) or CT coronary angiography as appropriate to pretest probability.
- Invasive coronary angiography when indicated (high-risk ACS, refractory ischemia, large area at risk, cardiogenic shock). ([European Society of Cardiology][4])
6) Important differentials
GERD/oesophagitis, pulmonary embolism, pericarditis, aortic dissection, musculoskeletal chest pain, panic/anxiety, pneumonia — use ECG, troponin, CXR, d-dimer/CT-PE and clinical exam to differentiate.
7) Management — overview (stepwise)
A. Initial resuscitation & early treatment (applies to all suspected ACS)
- ABCs, monitor, IV access; give chewable aspirin immediately (unless absolute contraindication). ([PubMed Central][5])
- Give anti-ischemic therapy: nitrates (sublingual GTN) for pain, IV morphine only if needed, oxygen only if SaO₂ <90%.
- Obtain 12-lead ECG and troponin promptly.
- Consider dual antiplatelet therapy (DAPT) and anticoagulation based on ACS subtype and planned invasive strategy (see below). ([European Society of Cardiology][4])
B. Reperfusion strategy for STEMI
- Primary percutaneous coronary intervention (PCI) at a PCI-capable center is preferred if it can be performed within guideline time targets (ideal door-to-balloon within recommended time windows). If PCI not available in a timely fashion, give fibrinolytic therapy (when no contraindications) ideally within 30 minutes of hospital arrival. Rescue PCI if fibrinolysis fails. ([European Society of Cardiology][4])
C. Management of NSTEMI / unstable angina
- Risk stratify (e.g., GRACE score). High-risk patients → early invasive strategy with coronary angiography and revascularization as indicated. Low-risk → conservative strategy with noninvasive testing and medical therapy. ([PubMed][6])
D. Long-term (secondary prevention, chronic coronary/CCS)
- Antiplatelet therapy: lifelong aspirin for most with established ASCVD; add P2Y12 inhibitor (clopidogrel/ticagrelor/prasugrel) as DAPT for defined durations after ACS/PCI (individualize bleeding vs ischemic risk). ([PubMed][7])
- High-intensity statin (e.g., atorvastatin 40–80 mg or rosuvastatin 20–40 mg) for secondary prevention unless contraindicated, with LDL-C goals and escalation/add-on therapies if needed. ([American Heart Association Journals][8])
- Beta-blocker, ACE inhibitor/ARB, mineralocorticoid antagonist when indicated (HF, LVEF ≤40%, HTN, diabetes), BP and diabetes control, smoking cessation, cardiac rehab, diet/exercise. ([PubMed][7])
8) Non-pharmacologic measures & prevention
- Smoking cessation (most impactful modifiable risk factor).
- Cardiac rehabilitation (exercise training, education, psychological support).
- Control blood pressure, glycaemia and lipids; weight reduction and Mediterranean-style diet; regular aerobic exercise.
- Vaccinations (influenza, pneumococcal as appropriate). ([World Health Organization][2])
9) Focused medication guide (main drugs used in IHD & ACS)
Below are practical summaries for the common drugs used in IHD. For each I include: indication, mechanism, typical adult dosing (and pediatric comments where relevant), PK/notes, common & serious adverse effects, major contraindications, key interactions, monitoring and patient counselling.
> Note: Pediatric dosing is generally not applicable for most IHD medications because coronary atherosclerotic disease is rare in children; when used (rarely) dosing is specialist-directed — I note this below where relevant.
Aspirin (acetylsalicylic acid)
- Indication: Immediate antiplatelet for suspected ACS; long-term secondary prevention of ASCVD.
- Mechanism: Irreversible COX-1 inhibition → reduced thromboxane A₂ → decreased platelet aggregation.
- Usual dosing: Loading in ACS: chewable 150–325 mg once (many guidelines recommend 160–325 mg or 150–300 mg initially). Maintenance: 75–100 mg daily. ([PubMed Central][5])
- PK: Rapid GI absorption; irreversible platelet COX inhibition for platelet lifetime (~7–10 days).
- Common AEs: GI upset, dyspepsia, bleeding (GI), allergic reactions (rare). Serious: GI bleed, hemorrhagic stroke (rare).
- Contraindications: Active major bleeding, known aspirin allergy (e.g., true anaphylaxis), hemorrhagic stroke.
- Interactions: Increased bleeding with anticoagulants, SSRIs; NSAIDs can reduce cardioprotective effect if taken concurrently (timing matters).
- Monitoring: Signs of bleeding, hemoglobin if concern; renal function if long-term and with other nephrotoxics.
- Counselling: Chew the initial dose for faster action in ACS; take maintenance dose regularly; report any black stools, bleeding gums, bruising, or severe stomach pain.
P2Y12 inhibitors — Clopidogrel, Ticagrelor, Prasugrel
- Indication: Add to aspirin as DAPT in ACS and after PCI; choice depends on bleeding risk, planned PCI, and specific contraindications. ([JACC][9])
Clopidogrel
- Mechanism: Irreversible P2Y12 ADP receptor blocker (prodrug requiring hepatic activation).
- Dosing (adult): Loading 300–600 mg (600 mg often used for PCI/STEMI), maintenance 75 mg daily. Pediatric: not routinely used for primary IHD in children; specialist dosing if indicated. ([PubMed][10])
- PK: Variable activation (CYP2C19), genetic polymorphisms affect effectiveness.
- AEs: Bleeding, rarely TTP.
- Contraindications: Active bleeding, severe hepatic impairment (caution).
- Interactions: Proton pump inhibitors (omeprazole) may reduce activation (avoid if possible); other CYP2C19 inhibitors alter effect.
- Monitoring: Watch for bleeding; consider platelet function/genotype testing in selected cases.
- Counselling: Take daily; missing doses increases risk of stent thrombosis.
Ticagrelor
- Mechanism: Reversible P2Y12 inhibitor (non-prodrug).
- Dosing: Loading 180 mg; maintenance 90 mg twice daily (or 60 mg twice daily after 12 months in some regimens/indications per guidelines).
- AEs: Dyspnea (common), bradyarrhythmia, bleeding.
- Contraindications/Interactions: Avoid with strong CYP3A inhibitors/inducers; avoid in active bleeding.
- Monitoring/Counselling: Advise about possible dyspnea; take twice daily; avoid strong CYP3A modulators.
Prasugrel
- Mechanism: Irreversible P2Y12 inhibitor (prodrug).
- Dosing: Loading 60 mg; maintenance 10 mg daily (5 mg if age ≥75 or body weight <60 kg — many centres use caution/avoid in older patients). Not recommended if history of stroke/TIA.
- AEs: Increased bleeding compared with clopidogrel in some subgroups.
- Contraindications: Prior stroke/TIA; high bleed risk.
- Use consideration: Preferred in some PCI populations (younger, stent patients without prior stroke) per some guidelines. ([JACC][9])
Unfractionated heparin (UFH) & Low molecular weight heparin (enoxaparin)
- Indication: Anticoagulation during ACS, peri-PCI, and with fibrinolysis protocols.
- UFH dosing (adult): bolus 60 IU/kg (max ~4,000 IU) followed by infusion 12 IU/kg/h (example for fibrinolysis adjunct); for PCI dosing different — follow local protocol. Monitor aPTT. ([Empendium][11])
- Enoxaparin: Weight-based dosing (e.g., 1 mg/kg SC q12h or 30 mg IV bolus + 1 mg/kg SC for some STEMI protocols); renal adjustment required.
- PK: Rapid onset (UFH), LMWH predictable PK but renally excreted.
- AEs: Bleeding, heparin-induced thrombocytopenia (HIT) (UFH > LMWH).
- Monitoring: aPTT for UFH; anti-Xa when needed for LMWH in renal dysfunction, obesity, or pregnancy.
- Contraindications: Active bleeding, severe thrombocytopenia, history of HIT (UFH), severe bleeding risk.
- Counselling: Bruising at injection site for LMWH; report any unusual bleeding or new rash.
Fibrinolytic therapy — Alteplase (tPA) (used when PCI not available timely in STEMI)
- Indication: Pharmacologic reperfusion in STEMI when timely PCI unavailable and no contraindications to thrombolysis.
- Mechanism: Plasminogen → plasmin → fibrin clot breakdown.
- Adult dosing (accelerated 90-minute regimen commonly used): 15 mg IV bolus, then 0.75 mg/kg (max 50 mg) over 30 minutes, then 0.5 mg/kg (max 35 mg) over 60 minutes; total dose ≤100 mg. (Alternate 3-hour regimens exist; follow local protocol). ([NCBI][12])
- PK/notes: Rapid fibrinolysis, short plasma half-life; combined with antiplatelet and anticoagulant therapy as per protocol.
- AEs: Major bleeding, intracranial hemorrhage (most feared), allergic reactions.
- Contraindications: Recent stroke, active internal bleeding, recent major surgery/trauma, uncontrolled hypertension, known bleeding diathesis (absolute/relative — follow guideline checklist). ([NCBI][12])
- Monitoring: Neurological status, hemoglobin/hematocrit, signs of bleeding; plan for urgent angiography if reperfusion fails.
- Counselling: Risks and benefits must be explained; thrombolysis carries bleeding risk including ICH.
Nitrates (Sublingual glyceryl trinitrate / GTN)
- Indication: Acute relief of ischemic chest pain and symptom control in stable angina.
- Mechanism: NO donor → venodilation → reduced preload and myocardial oxygen demand; coronary vasodilation to some degree.
- Dosing: Sublingual 0.3–0.6 mg (or 400–800 mcg) every 5 min up to 3 doses for acute pain; topical/IV options inpatient.
- AEs: Headache, hypotension, reflex tachycardia.
- Contraindications: Concomitant use of phosphodiesterase-5 inhibitors (e.g., sildenafil) within recommended washout period; severe hypotension; right ventricular infarction caution.
- Monitoring/Counselling: Sit when taking SL GTN; if no improvement after 2–3 doses or if hypotension, seek emergency care.
Beta-blockers (example: Metoprolol)
- Indication: Early beta-blocker therapy is standard after MI (unless contraindicated) to reduce ischemia, arrhythmia risk and mortality benefit in selected patients; chronic therapy for angina and LVEF reduction.
- Mechanism: β1 blockade → ↓heart rate, ↓contractility → ↓myocardial O₂ demand.
- Dosing: IV/PO regimens for acute MI vary; common oral starting doses (metoprolol succinate ER 25–50 mg once daily, titrate up to 100–200 mg daily as tolerated). IV bolus dosing (e.g., 5 mg IV over several minutes) used in some settings — follow protocol. ([NCBI][13])
- AEs: Fatigue, bradycardia, hypotension, bronchospasm in reactive airways disease (use cardioselective agents with caution).
- Contraindications: Severe bradycardia, high-degree heart block without pacemaker, decompensated heart failure (unless being treated), cardiogenic shock.
- Monitoring: Heart rate, blood pressure; ECG if arrhythmia.
- Counselling: Don’t stop abruptly (risk of angina/arrhythmia rebound); report dizziness, syncope, wheeze.
ACE inhibitors / ARBs (e.g., Ramipril)
- Indication: Post-MI with LV systolic dysfunction, hypertension, diabetic patients; reduce remodeling and mortality.
- Dosing: Ramipril start 2.5 mg once daily, titrate to 5–10 mg daily as tolerated (regimens vary).
- AEs: Cough (ACEi), hyperkalemia, renal dysfunction, angioedema (rare).
- Contraindications: Pregnancy, bilateral renal artery stenosis (relative/absolute), prior ACEi angioedema.
- Monitoring: Serum creatinine and potassium 1–2 weeks after initiation/titration.
- Counselling: Report cough, swelling of face/lips/tongue (angioedema), dizziness on standing.
High-intensity statins (Atorvastatin, Rosuvastatin)
- Indication: Secondary prevention in all patients with clinical ASCVD (including prior MI), with goal LDL-C lowering ≥50% and often LDL targets per guideline/region. ([American Heart Association Journals][8])
- Dosing: Atorvastatin 40–80 mg daily; Rosuvastatin 20–40 mg daily.
- PK: Oral, hepatic metabolism (CYP3A4 for atorvastatin), long half-life (rosuvastatin longer).
- AEs: Myalgia, elevated transaminases, rare rhabdomyolysis.
- Contraindications: Active liver disease, pregnancy/breastfeeding.
- Interactions: CYP3A4 inhibitors (for atorvastatin) increase statin levels; fibrates (gemfibrozil) increase myopathy risk.
- Monitoring: Baseline LFTs and CK if muscle symptoms; lipid panel 4–12 weeks after start/titration then every 3–12 months.
- Counselling: Take at night (some statins) but atorvastatin/rosuvastatin can be anytime; report unexplained muscle pain/weakness, brown urine.
Aldosterone antagonists (e.g., Spironolactone)
- Indication: Post-MI with LVEF ≤40% plus symptoms or diabetes, to reduce mortality; used in HFrEF.
- Dosing: Spironolactone 25–50 mg daily (individualize).
- AEs: Hyperkalemia, gynecomastia (spironolactone).
- Monitoring: Serum potassium and creatinine 3 days and 1 week after start, then periodically.
- Contraindications: Hyperkalemia, severe renal dysfunction.
10) Duration of dual antiplatelet therapy (DAPT)
- Typical DAPT after ACS/PCI is 12 months (aspirin + P2Y12 inhibitor), but duration should be individualized balancing ischemic vs bleeding risk (shorter or longer durations used depending on stent type, bleeding history, comorbidities). Newer guidelines and 2025 updates nuance P2Y12 choice and individualized duration. ([JACC][9])
11) Revascularization decisions
- PCI (percutaneous coronary intervention): First-line for reperfusion in STEMI if timely; used for diagnostic and therapeutic management in NSTEMI/high-risk ACS and in many patients with stable CCS when symptoms or ischemia burden warrant.
- CABG (coronary artery bypass grafting): Preferred in complex multivessel disease (e.g., left main disease, 3-vessel disease with LV dysfunction or diabetes) based on heart team assessment. ([European Society of Cardiology][4])
12) Prognosis & follow-up
- Early reperfusion and guideline-directed medical therapy reduce mortality after ACS. Long-term outcomes depend on extent of CAD, LV function, comorbidities, adherence to secondary prevention and lifestyle modification. Cardiac rehabilitation improves functional status and long-term outcomes. ([PubMed][7])
13) Key guideline & review links (authoritative external links)
- ESC Guidelines — Chronic Coronary Syndromes (diagnosis & long-term management). ([European Society of Cardiology][14])
- ESC Guidelines — Acute Coronary Syndromes (ACS) guidance and reperfusion/antithrombotic strategies. ([European Society of Cardiology][4])
- AHA/ACC Guideline — Chronic Coronary Disease / secondary prevention (2023). ([PubMed][7])
- StatPearls / NCBI chapters for drug & fibrinolysis dosing details (alteplase dosing summary). ([NCBI][12])
- Heart.org (American Heart Association patient/professional resources on ischemic heart disease and silent ischemia). ([www.heart.org][3])
> If you want, I can place these links as clickable URLs in a printable single-page PDF or a web-ready HTML summary (you previously told me you prefer single-file HTML/CSS/JS outputs) — say the word and I’ll generate that file for download.
14) Quick clinical checklists (useful at bedside)
Suspected STEMI: ABCs → ECG in ≤10 min → chewable aspirin immediately → call PCI team (if available) → if PCI not timely, consider fibrinolysis (check contraindications) → adjunctive antiplatelet/anticoagulant per protocol. ([European Society of Cardiology][4])
NSTEMI/UA: Evaluate hemodynamic stability → ECG + troponin serials → risk stratify (GRACE) → early invasive strategy for high risk; medical therapy + outpatient testing for low risk. ([PubMed][6])
15) What I did not include in exhaustive depth (and offer to expand)
I provided full, practical coverage and detailed drug summaries for the most commonly used agents in IHD/ACS. There are many additional medicines, procedures and nuanced situations (pregnancy, severe renal disease, complex antithrombotic de-escalation strategies, genetic testing for clopidogrel metabolism, novel lipid-lowering agents like PCSK9 inhibitors or inclisiran, advanced heart-failure devices and structural revascularization decisions) that I can expand into dedicated subsections with dosing, cost/availability and local guideline variants if you want — tell me which specific topics you want deeper (e.g., PCSK9 inhibitors, anticoagulant protocols in renal failure, DAPT de-escalation, pregnancy and IHD, or complete stepwise STEMI flowchart).
If you’d like:
- I can convert this into a single printable HTML file (formatted for your site/app) or a PDF with the references linked — which would be useful for your Medical Knowledge Hub.
- Or I can produce FAQ JSON and MCQ JSON sets on IHD (you’ve asked for those formats before) for use in quizzes — tell me which format (e.g., 15 hard case-based MCQs + 10 FAQs) and I’ll generate them next.
Would you like the printable single-file HTML or the MCQ/FAQ JSON next?
[1]: https://www.ncbi.nlm.nih.gov/books/NBK209964/?utm_source=chatgpt.com "Ischemic Heart Disease - Cardiovascular Disability - NCBI - NIH"
[2]: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-%28cvds%29?utm_source=chatgpt.com "Cardiovascular diseases (CVDs)"
[3]: https://www.heart.org/en/health-topics/heart-attack/about-heart-attacks/silent-ischemia-and-ischemic-heart-disease?utm_source=chatgpt.com "Ischemic Heart Disease and Silent Ischemia"
[4]: https://www.escardio.org/Guidelines/Clinical-Practice-Guidelines/Acute-Coronary-Syndromes-ACS-Guidelines?utm_source=chatgpt.com "2023 ESC Guidelines for the management of acute ..."
[5]: https://pmc.ncbi.nlm.nih.gov/articles/PMC4107436/?utm_source=chatgpt.com "Oral Antiplatelet Therapy in Acute Coronary Syndromes"
[6]: https://pubmed.ncbi.nlm.nih.gov/32860058/?utm_source=chatgpt.com "2020 ESC Guidelines for the management of acute ..."
[7]: https://pubmed.ncbi.nlm.nih.gov/37471501/?utm_source=chatgpt.com "2023 AHA/ACC/ACCP/ASPC/NLA/PCNA Guideline ... - PubMed"
[8]: https://www.ahajournals.org/doi/10.1161/cir.0000000000000625?utm_source=chatgpt.com "2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/ ..."
[9]: https://www.jacc.org/doi/10.1016/j.jacc.2025.04.002?utm_source=chatgpt.com "Antiplatelet and Anticoagulant Therapy in the 2025 ACC ..."
[10]: https://pubmed.ncbi.nlm.nih.gov/16563901/?utm_source=chatgpt.com "Clopidogrel loading dose (300 versus 600 mg) strategies ..."
[11]: https://empendium.com/mcmtextbook/table/B31.2.5-8.?utm_source=chatgpt.com "Fibrinolysis in patients with STEMI - McMaster Textbook of ..."
[12]: https://www.ncbi.nlm.nih.gov/books/NBK499977/?utm_source=chatgpt.com "Alteplase - StatPearls - NCBI Bookshelf - NIH"
[13]: https://www.ncbi.nlm.nih.gov/books/NBK532923/?utm_source=chatgpt.com "Metoprolol - StatPearls - NCBI Bookshelf"
[14]: https://www.escardio.org/Guidelines/Clinical-Practice-Guidelines/Chronic-Coronary-Syndromes?utm_source=chatgpt.com "ESC Guidelines for the management of chronic coronary ..."
Below is a single, exhaustive, clinically oriented reference with 30 detailed differential case scenarios related to Ischemic Heart Disease (IHD).
For each case, I provide:
- Clinical scenario
- Most likely diagnosis (differential)
- Key distinguishing points
- Detailed management (stepwise)
- Major contraindications / cautions
No images included, as requested.
ISCHEMIC HEART DISEASE
30 Differential Case Scenarios With Detailed Management and Contraindications
1. Stable Angina
Scenario:
55-year-old man with exertional chest tightness relieved by rest, predictable pattern.
Diagnosis: Stable angina (fixed coronary stenosis)
Key points:
- Demand–supply mismatch
- Normal troponin
- Stress test positive
Management:
- Aspirin 75–100 mg daily
- Beta-blocker (first line)
- High-intensity statin
- Nitrates for symptom relief
- Risk-factor modification
- Consider PCI if refractory
Contraindications:
- Beta-blockers: severe asthma, AV block
- Nitrates: hypotension, PDE-5 inhibitors
2. Unstable Angina
Scenario:
Chest pain at rest, increasing frequency, normal troponin.
Diagnosis: Unstable angina
Management:
- Hospital admission
- Aspirin + P2Y12 inhibitor
- Anticoagulation (UFH/LMWH)
- Early invasive strategy if high risk
Contraindications:
- Thrombolysis is contraindicated
- NSAIDs increase mortality
3. NSTEMI
Scenario:
Chest pain with ST depression and positive troponin.
Diagnosis: NSTEMI
Management:
- Dual antiplatelet therapy
- Anticoagulation
- Beta-blocker, statin, ACE inhibitor
- Early angiography
Contraindications:
- Thrombolysis contraindicated
- Avoid prasugrel before angiography if anatomy unknown
4. STEMI (Anterior Wall)
Scenario:
Severe chest pain with ST elevation V1–V4.
Diagnosis: Anterior STEMI
Management:
- Primary PCI preferred
- If unavailable → thrombolysis
- DAPT + anticoagulation
- ICU monitoring
Contraindications:
- Thrombolysis contraindicated if prior hemorrhagic stroke
- Beta-blockers avoided in shock
5. Inferior STEMI With RV Involvement
Scenario:
Inferior ST elevation, hypotension, raised JVP, clear lungs.
Diagnosis: RV infarction
Management:
- IV fluids
- Primary PCI
- Avoid nitrates and diuretics
Contraindications:
- Nitrates → severe hypotension
- Morphine cautiously
6. Silent Ischemia
Scenario:
Diabetic patient with ischemic ECG changes, no chest pain.
Diagnosis: Silent myocardial ischemia
Management:
- Aggressive medical therapy
- Statins, antiplatelets
- Revascularization if high ischemic burden
Contraindications:
- None specific; high vigilance required
7. Prinzmetal (Variant) Angina
Scenario:
Chest pain at rest, transient ST elevation, relieved by nitrates.
Diagnosis: Coronary vasospasm
Management:
- Calcium channel blockers
- Long-acting nitrates
- Smoking cessation
Contraindications:
- Beta-blockers worsen spasm
8. Microvascular Angina
Scenario:
Angina with normal coronary angiography.
Diagnosis: Microvascular dysfunction
Management:
- Beta-blockers
- ACE inhibitors
- Statins
- Lifestyle therapy
Contraindications:
- PCI not beneficial
9. Acute Pericarditis
Scenario:
Sharp chest pain relieved by sitting forward, diffuse ST elevation.
Differential from IHD
Management:
- NSAIDs
- Colchicine
Contraindications:
- Thrombolysis contraindicated
- Anticoagulation increases tamponade risk
10. Aortic Dissection
Scenario:
Tearing chest pain radiating to back, BP differential.
Differential
Management:
- Immediate BP control (beta-blocker)
- Emergency surgery
Contraindications:
- Thrombolysis absolutely contraindicated
11. Pulmonary Embolism
Scenario:
Sudden dyspnea, pleuritic pain, tachycardia.
Management:
- Anticoagulation
- Thrombolysis if massive PE
Contraindications:
- Antiplatelets alone insufficient
12. Takotsubo Cardiomyopathy
Scenario:
Post-emotional stress, ST elevation, normal coronaries.
Management:
- Supportive
- Beta-blockers
- ACE inhibitors
Contraindications:
- Inotropes if LV outflow obstruction
13. Post-MI Papillary Muscle Rupture
Scenario:
Acute pulmonary edema, new systolic murmur.
Management:
- Urgent surgery
- Vasodilators, IABP
Contraindications:
- Delay is fatal
14. Ventricular Septal Rupture
Scenario:
Shock, harsh holosystolic murmur.
Management:
- Emergency surgical repair
- IABP
Contraindications:
- Medical therapy alone
15. Free Wall Rupture
Scenario:
Sudden collapse, tamponade signs.
Management:
- Emergency pericardiocentesis
- Surgery
Contraindications:
- Anticoagulation
16. Dressler Syndrome
Scenario:
Weeks after MI, fever, pleuritic pain.
Management:
- NSAIDs
- Colchicine
Contraindications:
- Steroids early post-MI (unless refractory)
17. Ischemic Cardiomyopathy
Scenario:
Chronic heart failure after MI.
Management:
- GDMT for HFrEF
- ICD if EF ≤35%
- CABG if viable myocardium
Contraindications:
- Non-dihydropyridine CCBs
18. Post-MI Ventricular Aneurysm
Scenario:
Persistent ST elevation weeks later.
Management:
- Anticoagulation
- Surgery if refractory
Contraindications:
- Thrombolysis
19. Acute Stent Thrombosis
Scenario:
Sudden chest pain after PCI.
Management:
- Emergency PCI
- IV antiplatelets
Contraindications:
- Stopping DAPT
20. In-Stent Restenosis
Scenario:
Recurrent angina months after PCI.
Management:
- Repeat PCI
- Drug-coated balloon
Contraindications:
- Balloon angioplasty alone (high recurrence)
21. Cardiogenic Shock
Scenario:
Hypotension, cold extremities post-MI.
Management:
- Emergency PCI
- Vasopressors
- Mechanical support
Contraindications:
- Beta-blockers acutely
22. Arrhythmias After MI (VT/VF)
Scenario:
Sudden collapse post-MI.
Management:
- Defibrillation
- Amiodarone
- ICD later
Contraindications:
- Class IC antiarrhythmics
23. Inferior MI With AV Block
Scenario:
Bradycardia, hypotension.
Management:
- Atropine
- Temporary pacing if needed
Contraindications:
- Early permanent pacemaker
24. Late Presenter STEMI
Scenario:
24 hours post-MI, pain-free.
Management:
- Optimal medical therapy
- No routine PCI
Contraindications:
- Thrombolysis
25. Cocaine-Induced Ischemia
Scenario:
Chest pain after cocaine use.
Management:
- Benzodiazepines
- Nitrates
- CCBs
Contraindications:
- Beta-blockers (unopposed alpha effect)
26. Anemia-Induced Ischemia
Scenario:
Angina with Hb 6 g/dL.
Management:
- Blood transfusion
- Treat cause
Contraindications:
- PCI before correcting anemia
27. Hypertensive Emergency With Ischemia
Scenario:
Severe BP elevation with chest pain.
Management:
- IV nitrates
- Beta-blockers
Contraindications:
- Rapid BP overcorrection
28. Chronic Kidney Disease With IHD
Scenario:
IHD in ESRD patient.
Management:
- Medical therapy
- PCI cautiously
Contraindications:
- Excess contrast use
- NSAIDs
29. Elderly With Frailty
Scenario:
85-year-old with NSTEMI.
Management:
- Individualized invasive approach
- Bleeding risk assessment
Contraindications:
- Aggressive antithrombotics without assessment
30. Pregnancy With Ischemia
Scenario:
Pregnant woman with chest pain.
Management:
- Aspirin (low dose)
- Beta-blockers (labetalol)
- Multidisciplinary care
Contraindications:
- ACE inhibitors
- Statins
- Warfarin