Respiratory System Physiology
Primary Functions
- Gas exchange – O₂ uptake and CO₂ elimination
- Acid–base regulation – via control of PaCO₂
- Phonation – airflow for speech
- Defense – filtration, mucociliary clearance, immune cells
- Metabolic functions – ACE production, inactivation of vasoactive substances
- Thermoregulation & water balance
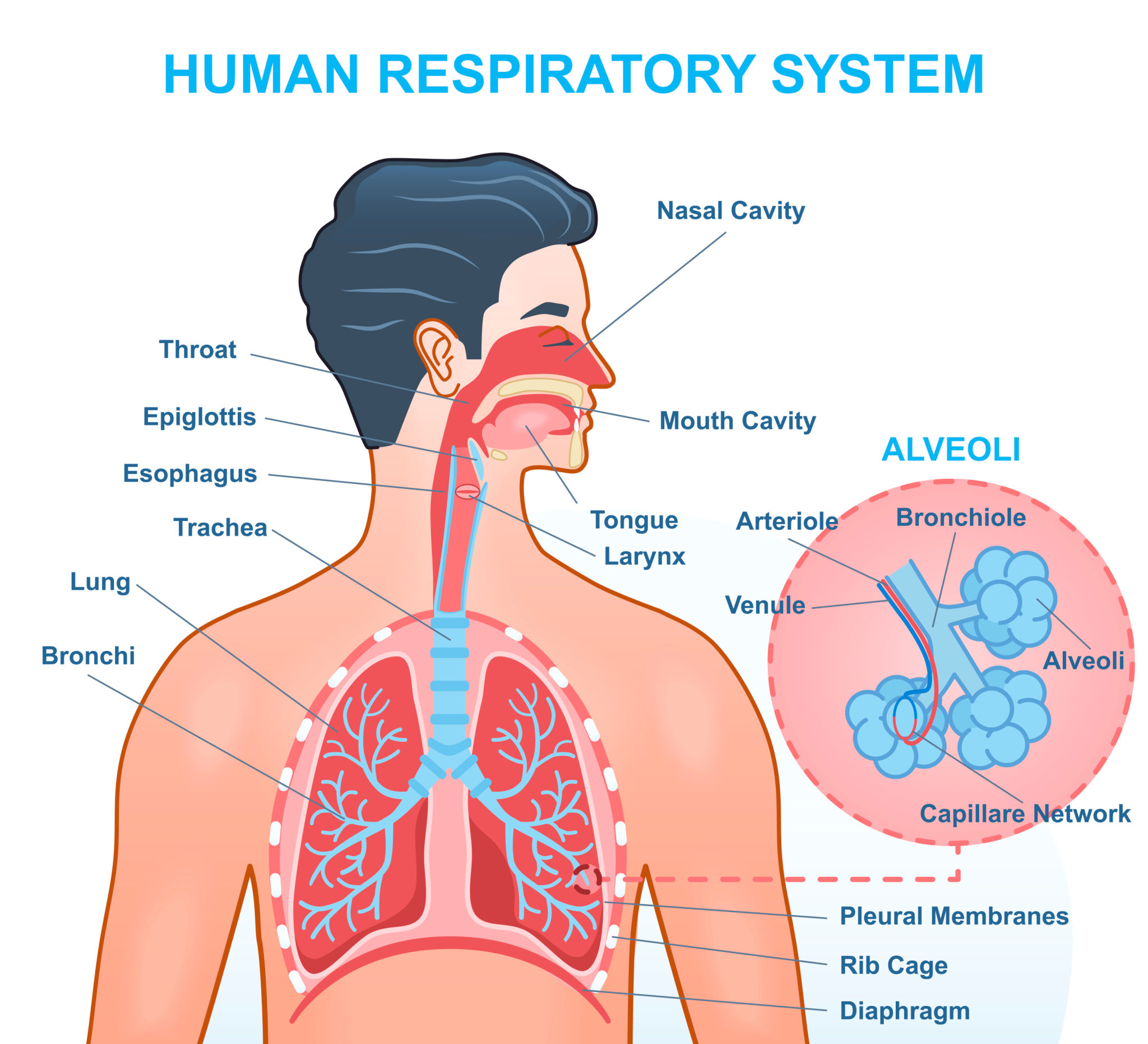
Anatomical–Functional Divisions
- Conducting zone
* Nose → pharynx → larynx → trachea → bronchi → terminal bronchioles
* No gas exchange
* Functions: warming, humidifying, filtering air
- Respiratory zone
* Respiratory bronchioles → alveolar ducts → alveoli
* Site of gas exchange
Mechanics of Breathing (Pulmonary Ventilation)
Inspiration (Active)
- Diaphragm contracts → moves downward
- External intercostals elevate ribs
- Thoracic volume ↑ → intrapleural pressure becomes more negative
- Alveolar pressure ↓ (≈ –1 cm H₂O) → air flows in
Expiration
- Quiet expiration: passive (elastic recoil)
- Forced expiration: active (internal intercostals + abdominal muscles)
Pressures Involved
| Pressure | Normal Value |
| ----------------------- | ------------ |
| Atmospheric pressure | 760 mmHg |
| Intrapleural pressure | –5 cm H₂O |
| Alveolar pressure | 0 cm H₂O |
| Transpulmonary pressure | +5 cm H₂O |
Lung Compliance
- Definition: ΔVolume / ΔPressure
- High compliance: emphysema
- Low compliance: fibrosis, ARDS
- Determined by:
* Elastic tissue
* Alveolar surface tension
Surfactant
- Secreted by Type II pneumocytes
- Reduces surface tension
- Prevents alveolar collapse (atelectasis)
- Increases lung compliance
- Deficiency → neonatal respiratory distress syndrome
Airway Resistance
- Greatest in medium-sized bronchi
- Influenced by:
* Airway radius (most important)
* Lung volume
* Smooth muscle tone
- Bronchodilation: sympathetic (β₂)
- Bronchoconstriction: parasympathetic (M₃)
Lung Volumes and Capacities
Volumes
- Tidal Volume (TV) ≈ 500 mL
- Inspiratory Reserve Volume (IRV)
- Expiratory Reserve Volume (ERV)
- Residual Volume (RV)
Capacities
- Vital Capacity (VC = TV + IRV + ERV)
- Total Lung Capacity (TLC = VC + RV)
- Functional Residual Capacity (FRC = ERV + RV)
Alveolar Ventilation
[
V_A = (V_T – V_D) × f
]
- Dead space ≈ 150 mL
- Alveolar ventilation determines PaCO₂
Diffusion of Gases
- Governed by Fick’s law
- Factors:
* Surface area
* Thickness of membrane
* Partial pressure gradient
* Diffusion coefficient
Partial Pressures (mmHg)
| Location | O₂ | CO₂ |
| --------------- | --- | --- |
| Atmospheric air | 160 | 0.3 |
| Alveoli | 104 | 40 |
| Arterial blood | 95 | 40 |
| Venous blood | 40 | 46 |
Ventilation–Perfusion (V/Q) Ratio
- Normal ≈ 0.8
- High V/Q → dead space (pulmonary embolism)
- Low V/Q → shunt (pneumonia, asthma)
Transport of Oxygen
- Bound to hemoglobin (98%)
- Dissolved in plasma (2%)
Oxyhemoglobin Dissociation Curve
- Sigmoid shape
- Right shift (↓ affinity):
* ↑ CO₂
* ↑ H⁺ (↓ pH)
* ↑ Temperature
* ↑ 2,3-BPG
(Bohr effect)
Transport of Carbon Dioxide
- Bicarbonate (70%)
- Carbaminohemoglobin (23%)
- Dissolved CO₂ (7%)
Chloride Shift
- Exchange of HCO₃⁻ and Cl⁻ in RBCs
Control of Respiration
Respiratory Centers
- Medulla
* Dorsal respiratory group (inspiration)
* Ventral respiratory group (forced breathing)
- Pons
* Pneumotaxic center (rate control)
* Apneustic center (depth)
Chemoreceptors
Central Chemoreceptors
- Located in medulla
- Respond to ↑ CO₂ / ↓ pH
- Most powerful stimulus
Peripheral Chemoreceptors
- Carotid & aortic bodies
- Respond to:
* ↓ PaO₂ (< 60 mmHg)
* ↑ PaCO₂
* ↓ pH
Reflexes
- Hering–Breuer reflex – prevents overinflation
- Cough reflex – airway protection
- Sneezing reflex – nasal clearance
- J-receptor reflex – pulmonary congestion → dyspnea
Non-Respiratory Functions
- ACE converts angiotensin I → II
- Filtration of micro-emboli
- Immune defense (macrophages, IgA)
Key Clinical Correlations
- Hypoventilation → respiratory acidosis
- Hyperventilation → respiratory alkalosis
- COPD → ↓ PaO₂, ↑ PaCO₂
- Fibrosis → ↓ compliance
- Emphysema → ↑ compliance, ↓ elastic recoil