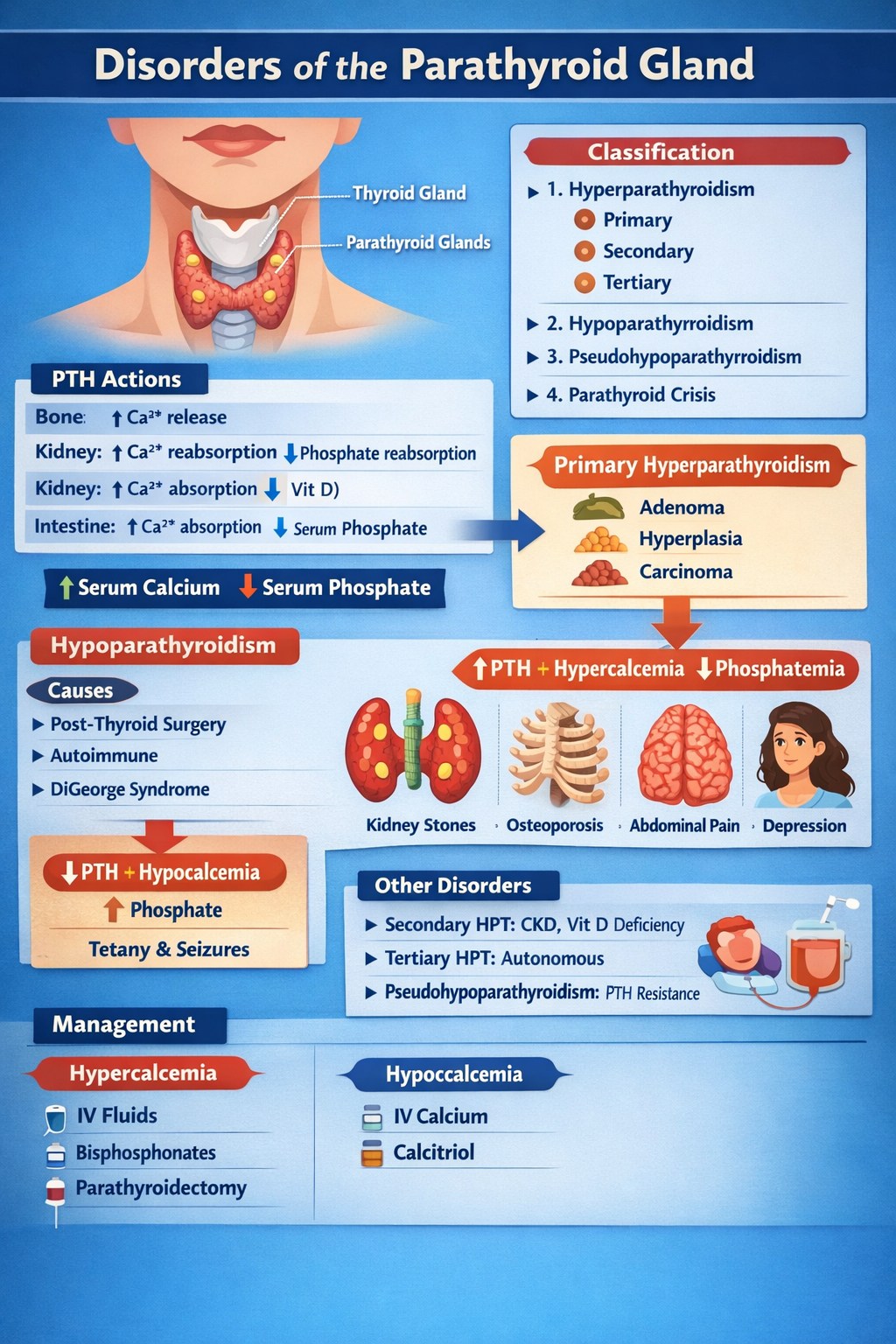
DISORDERS OF THE PARATHYROID GLAND
1. Physiology of Parathyroid Hormone (PTH)
Parathyroid glands (4) → secrete PTH → maintain serum calcium and phosphate balance
Normal actions of PTH
| Target organ | Action |
| ------------- | ----------------------------------------------- |
| Bone | ↑ Osteoclastic bone resorption → ↑ Ca²⁺ release |
| Kidney | ↑ Ca²⁺ reabsorption, ↓ phosphate reabsorption |
| Kidney | ↑ 1-α hydroxylase → ↑ calcitriol |
| Intestine | Indirectly ↑ Ca²⁺ absorption via vitamin D |
Net effect:
↑ Serum calcium, ↓ serum phosphate
CLASSIFICATION
- Hyperparathyroidism
* Primary
* Secondary
* Tertiary
- Hypoparathyroidism
- Pseudohypoparathyroidism
- Parathyroid crisis
PRIMARY HYPERPARATHYROIDISM (PHPT)
Definition
Autonomous excessive PTH secretion → hypercalcemia
Causes
| Cause | % |
| ----------------------- | ------ |
| Parathyroid adenoma | 85% |
| Parathyroid hyperplasia | 10–15% |
| Parathyroid carcinoma | <1% |
| MEN-1, MEN-2A | Rare |
Pathophysiology
Excess PTH →
- ↑ Bone resorption → osteoporosis
- ↑ Renal Ca reabsorption
- ↑ Vitamin D → ↑ gut Ca absorption
→ Hypercalcemia + hypophosphatemia
Clinical Features
“Stones, Bones, Groans, Thrones, Psychiatric Overtones”
| System | Features |
| ------ | ---------------------------------------------- |
| Kidney | Nephrolithiasis, polyuria |
| Bone | Bone pain, fractures, osteitis fibrosa cystica |
| GIT | Constipation, pancreatitis, peptic ulcer |
| CNS | Depression, confusion |
| Heart | Short QT |
Investigations
| Test | Result |
| -------------------- | ---------------- |
| Serum Ca | ↑ |
| Serum phosphate | ↓ |
| PTH | ↑ |
| ALP | ↑ |
| 24-hr urine Ca | ↑ |
| DEXA | Osteoporosis |
| Neck USG / Sestamibi | Localize adenoma |
Differential Diagnosis
| Condition | PTH | Ca |
| ------------------------ | --- | -------- |
| PHPT | ↑ | ↑ |
| Malignancy hypercalcemia | ↓ | ↑ |
| FHH | ↑ | Normal/↑ |
Management
A. Acute hypercalcemia
| Step | Treatment |
| ---- | ----------------- |
| 1 | IV normal saline |
| 2 | Loop diuretic |
| 3 | IV bisphosphonate |
| 4 | Calcitonin |
B. Definitive
Parathyroidectomy
Indications
- Ca >1 mg/dL above normal
- Kidney stones
- Osteoporosis
- Age <50
SECONDARY HYPERPARATHYROIDISM
Definition
Compensatory ↑ PTH due to hypocalcemia
Causes
- Chronic kidney disease (most common)
- Vitamin D deficiency
- Malabsorption
Biochemistry
| Parameter | Result |
| --------- | ---------- |
| Calcium | ↓ |
| Phosphate | ↑ (in CKD) |
| PTH | ↑ |
| Vitamin D | ↓ |
Management
- Oral calcium
- Vitamin D (calcitriol)
- Phosphate binders
- Dialysis if CKD
TERTIARY HYPERPARATHYROIDISM
Long-standing secondary → autonomous glands
| Ca | PTH |
| -- | --- |
| ↑ | ↑ |
Treatment: Parathyroidectomy
HYPOPARATHYROIDISM
Definition
Deficient PTH → hypocalcemia
Causes
- Post-thyroid surgery (most common)
- Autoimmune
- DiGeorge syndrome
- Hypomagnesemia
Pathophysiology
Low PTH → ↓ calcium, ↑ phosphate → neuromuscular excitability
Clinical Features
| Feature | Mechanism |
| --------------- | ------------------------------ |
| Tetany | Hypocalcemia |
| Chvostek sign | Facial nerve hyperexcitability |
| Trousseau sign | Carpopedal spasm |
| Seizures | Low Ca |
| QT prolongation | Hypocalcemia |
Investigations
| Test | Result |
| --------- | -------- |
| Ca | ↓ |
| Phosphate | ↑ |
| PTH | ↓ |
| Mg | May be ↓ |
Management
Acute
IV calcium gluconate
Chronic
- Oral calcium
- Calcitriol
CALCIUM GLUCONATE
| Parameter | Value |
| ------------ | -------------------- |
| Indication | Acute tetany |
| Mechanism | Raises serum Ca |
| Dose | 10 ml of 10% IV slow |
| Side effects | Arrhythmia |
| Monitoring | ECG |
CALCITRIOL (Vitamin D)
| Feature | Detail |
| ------------ | -------------------------- |
| Action | ↑ Intestinal Ca absorption |
| Dose | 0.25–1 mcg/day |
| Side effects | Hypercalcemia |
| Monitoring | Serum Ca |
PSEUDOHYPOPARATHYROIDISM
Definition
Target organ resistance to PTH
| Ca | PTH | Phosphate |
| -- | --- | --------- |
| ↓ | ↑ | ↑ |
Clinical
- Short stature
- Round face
- Brachydactyly
- Mental retardation
Treatment: Calcium + Vitamin D
PARATHYROID CRISIS
Severe hypercalcemia (>14 mg/dL)
Features
- Dehydration
- Arrhythmia
- Coma
Management
- IV saline
- Loop diuretic
- Calcitonin
- Bisphosphonates
- Dialysis if refractory
EXAM PEARLS
| Scenario | Diagnosis |
| --------------------------------- | --------------------------- |
| High Ca + high PTH | Primary hyperparathyroidism |
| Low Ca + high PTH | Secondary HPT |
| Low Ca + low PTH | Hypoparathyroidism |
| Low Ca + high PTH + short fingers | Pseudohypoparathyroidism |