Multifocal Atrial Tachycardia (MAT)
1. Definition
Multifocal atrial tachycardia (MAT) is a supraventricular tachyarrhythmia characterized by:
- Irregular atrial rhythm
- Heart rate > 100 beats/min
- At least three distinct P-wave morphologies on ECG
It reflects multiple ectopic atrial pacemakers firing independently.
2. Epidemiology
- Predominantly seen in elderly patients
- Strongly associated with severe pulmonary disease
- Common in hospitalized and critically ill patients
3. Pathophysiology
MAT results from enhanced atrial automaticity due to:
- Hypoxemia → ↑ sympathetic tone
- Hypercapnia and acidosis
- Atrial stretch
- Electrolyte disturbances
Multiple atrial foci compete with the sinus node → chaotic atrial depolarization → irregular ventricular response.
4. Common Causes and Triggers
Pulmonary Causes (most important)
- Chronic obstructive pulmonary disease (COPD)
- Acute exacerbation of asthma
- Pneumonia
- Pulmonary embolism
- Respiratory failure
Cardiac Causes
- Congestive heart failure
- Ischemic heart disease
- Valvular heart disease
Metabolic and Systemic Causes
- Hypoxia
- Hypokalemia
- Hypomagnesemia
- Sepsis
- Renal failure
Drug-Related
- Theophylline
- Beta-agonists
- Excess catecholamines
5. Clinical Features
Symptoms
- Palpitations
- Dyspnea
- Fatigue
- Lightheadedness
- Worsening respiratory distress
Signs
- Irregularly irregular pulse
- Tachycardia
- Features of underlying lung disease
- Possible hypotension in severe cases
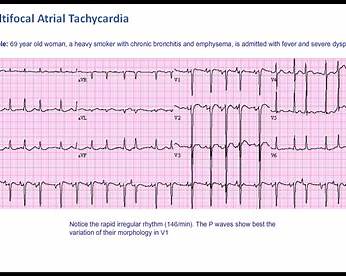
6. Electrocardiographic (ECG) Features
Diagnostic Criteria
- Heart rate > 100/min
- Irregularly irregular rhythm
- ≥ 3 different P-wave morphologies
- Variable PR intervals
- Isoelectric baseline between P waves (helps distinguish from atrial fibrillation)
7. Differential Diagnosis
| Condition | Key Distinguishing Feature |
| ---------------------------------- | --------------------------------- |
| Atrial fibrillation | No distinct P waves |
| Atrial flutter with variable block | Sawtooth flutter waves |
| Sinus tachycardia with PACs | Single P-wave morphology |
| Wandering atrial pacemaker | Same ECG pattern but HR < 100/min |
8. Investigations
Essential
- 12-lead ECG (diagnostic)
- Pulse oximetry / ABG
- Serum electrolytes (K⁺, Mg²⁺)
- Chest X-ray
- Renal function tests
Additional (if indicated)
- Echocardiography
- Cardiac biomarkers (if ischemia suspected)
9. Management (Stepwise and Definitive)
A. Treat the Underlying Cause (MOST IMPORTANT)
- Correct hypoxia → oxygen therapy
- Treat COPD/asthma exacerbation
- Manage infection or sepsis
- Correct electrolyte imbalance
- Stop offending drugs (e.g., theophylline)
> MAT rarely resolves unless the underlying cause is corrected
B. Rate Control (if symptomatic or hemodynamically unstable)
1. Magnesium Sulfate
- Indication: First-line therapy even if Mg²⁺ is normal
- Mechanism: Stabilizes atrial myocardium and suppresses ectopic activity
- Dose:
* IV 2 g over 10–15 minutes
- Adverse Effects: Hypotension, flushing (rare)
- Monitoring: Blood pressure, deep tendon reflexes
2. Calcium Channel Blockers (Preferred in COPD)
Verapamil or Diltiazem
- Mechanism: Slows AV nodal conduction
- Dose:
* Verapamil IV 2.5–5 mg slowly
* Diltiazem IV bolus followed by infusion
- Contraindications: Severe LV dysfunction, hypotension
- Adverse Effects: Bradycardia, hypotension
3. Beta-Blockers (Use with Caution)
- Mechanism: Reduce sympathetic drive
- Use: Only if no significant bronchospasm
- Contraindications: Severe COPD, asthma
C. What NOT to Use
- Digoxin: Ineffective
- Electrical cardioversion: Ineffective (automatic focus arrhythmia)
- Class I or III antiarrhythmics: Not recommended
10. Anticoagulation
- Not indicated
- Unlike atrial fibrillation, MAT does not increase thromboembolic risk
11. Prognosis
- MAT itself is not usually fatal
- Prognosis depends on the underlying disease
- High in-hospital mortality reflects severity of comorbid illness, not arrhythmia
12. Special Clinical Points
- MAT is often a marker of severe illness
- Always look for hypoxia or lung pathology
- Misdiagnosis as atrial fibrillation can lead to inappropriate anticoagulation
13. Exam-Oriented Summary
- Elderly + COPD + irregular tachycardia → think MAT
- ≥ 3 P-wave morphologies
- Treat cause first, not the rhythm
- Magnesium and calcium channel blockers are mainstays