CONGESTIVE HEART FAILURE (CHF)
1. Definition
Congestive Heart Failure is a clinical syndrome in which the heart is unable to pump sufficient blood to meet the metabolic demands of the body, or can do so only at elevated filling pressures, resulting in pulmonary and/or systemic congestion.
2. Classification
A. By Ejection Fraction
- HFrEF (Systolic HF): LVEF ≤ 40%
- HFmrEF: LVEF 41–49%
- HFpEF (Diastolic HF): LVEF ≥ 50%
B. By Side
- Left-sided HF → pulmonary congestion
- Right-sided HF → systemic venous congestion
- Biventricular HF
C. By Course
- Acute HF
- Chronic stable HF
- Acute decompensated HF (ADHF)
D. ACC/AHA Stages
- Stage A: Risk factors only
- Stage B: Structural disease, no symptoms
- Stage C: Structural disease with symptoms
- Stage D: Refractory end-stage HF
3. Pathophysiology
- Primary myocardial dysfunction
* Reduced contractility (HFrEF)
* Impaired relaxation/compliance (HFpEF)
- Reduced cardiac output
* ↓ renal perfusion → RAAS activation
* ↑ sympathetic nervous system
- Neurohormonal activation
* RAAS → Na⁺/H₂O retention → congestion
* SNS → tachycardia, vasoconstriction
* ADH → free water retention
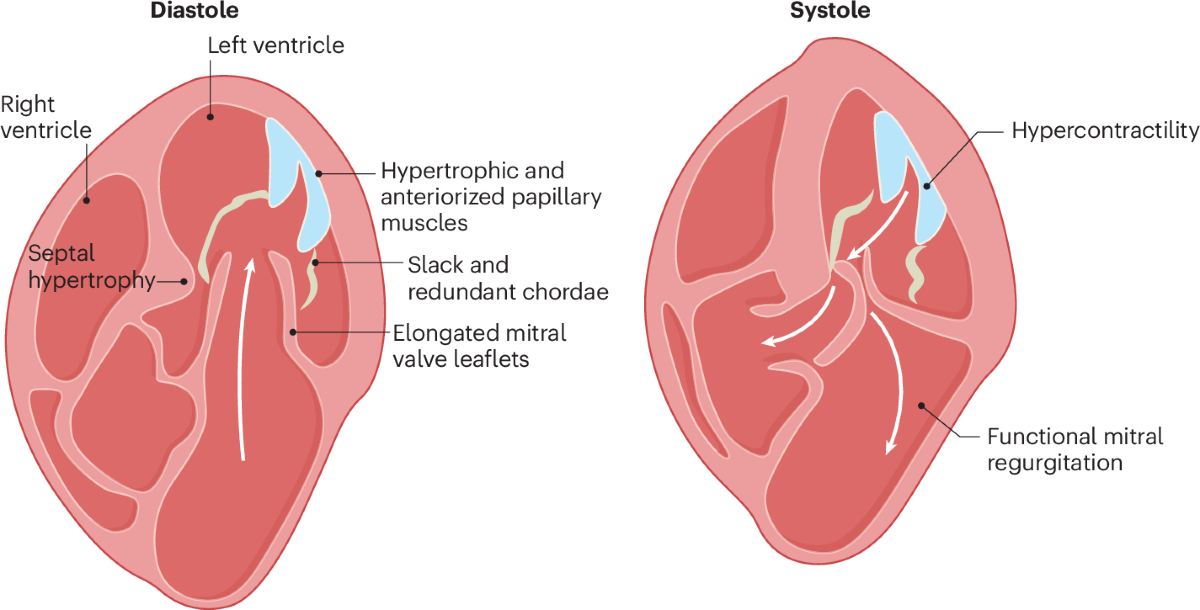
- Cardiac remodeling
* Ventricular dilation or hypertrophy
* Progressive decline in function
4. Etiology / Causes
Common Causes
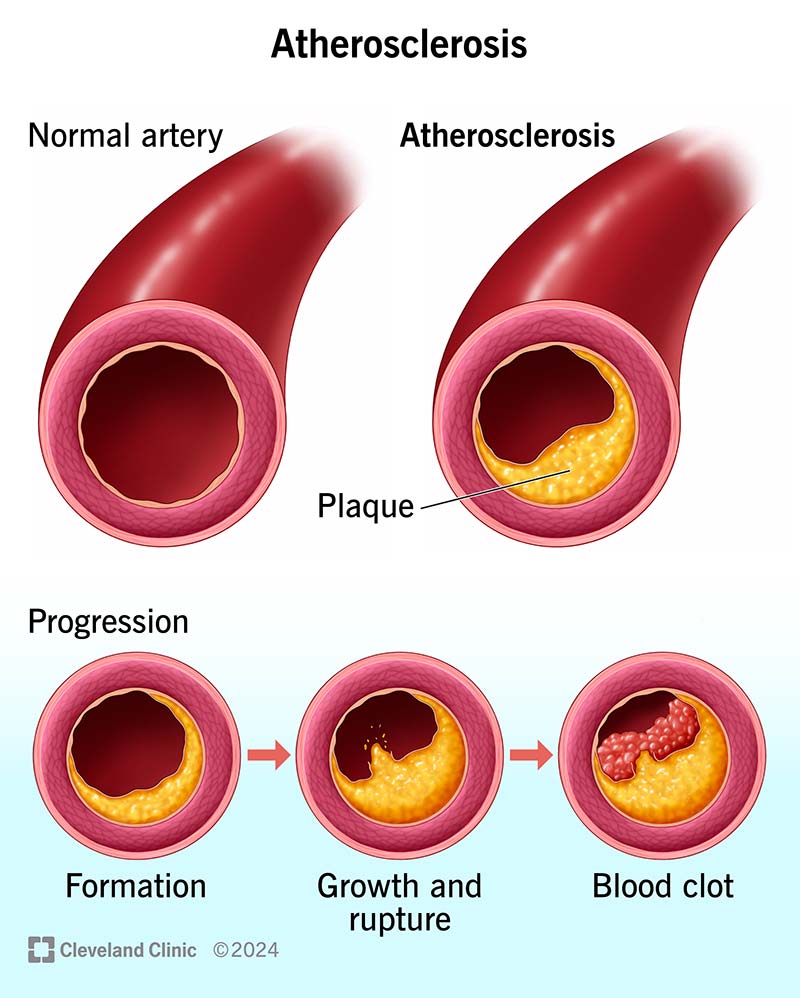
- Ischemic heart disease (most common)
- Hypertension
- Valvular heart disease
- Dilated cardiomyopathy
- Arrhythmias (AF, VT)
Other Causes
- Congenital heart disease
- Myocarditis
- Infiltrative diseases (amyloidosis)
- Endocrine: thyroid disease
- Toxins: alcohol, chemotherapy
- Peripartum cardiomyopathy
5. Precipitating / Decompensating Factors
- Infection
- Non-compliance with drugs/diet
- Acute coronary syndrome
- Uncontrolled hypertension
- Arrhythmias
- Renal failure
- NSAIDs, steroids, excess IV fluids
6. Clinical Features
Symptoms
- Dyspnea (exertional → rest)
- Orthopnea
- Paroxysmal nocturnal dyspnea
- Fatigue, weakness
- Reduced exercise tolerance
- Nocturia
- Weight gain
Signs
Left-sided HF
- Tachypnea
- Bibasilar crepitations
- S3 gallop
- Pulmonary edema
Right-sided HF
- Raised JVP
- Hepatomegaly
- Ascites
- Peripheral edema
7. Investigations / Diagnosis
Basic
- ECG: ischemia, LVH, arrhythmias
- Chest X-ray: cardiomegaly, pulmonary congestion
- Echocardiography (key test):
* LVEF
* Diastolic function
* Valvular disease
Laboratory
- BNP / NT-proBNP (↑)
- CBC (anemia)
- RFT, electrolytes
- LFT
- Thyroid profile
- HbA1c, lipid profile
Advanced (when indicated)
- Cardiac MRI
- Coronary angiography
- Stress testing
8. Differential Diagnosis
- COPD / asthma
- Pneumonia
- Pulmonary embolism
- Renal failure with fluid overload
- Constrictive pericarditis
- Cirrhosis with ascites
9. Management (Stepwise & Evidence-Based)
A. Non-Pharmacological Measures
- Salt restriction (<2 g/day)
- Fluid restriction (1.5–2 L/day)
- Daily weight monitoring
- Smoking and alcohol cessation
- Vaccination (influenza, pneumococcal)
- Exercise-based cardiac rehabilitation
B. Pharmacological Management (Chronic HFrEF)
1. ACE Inhibitors (or ARB if intolerant)
- Indication: All HFrEF patients
- Mechanism: RAAS inhibition → ↓ preload & afterload
- Example & Dose:
* Enalapril: start 2.5 mg BD → target 10–20 mg BD
- Adverse Effects: Cough, hyperkalemia, renal dysfunction
- Contraindications: Pregnancy, bilateral renal artery stenosis
- Monitoring: K⁺, creatinine
- Counseling: Report dizziness, avoid NSAIDs
2. ARNI (Preferred over ACEI/ARB)
- Drug: Sacubitril + Valsartan
- Indication: Symptomatic HFrEF despite ACEI/ARB
- Dose: Start 24/26 or 49/51 mg BD → target 97/103 mg BD
- Washout: 36 h after stopping ACEI
- Adverse: Hypotension, angioedema
3. Beta-Blockers (Evidence-based only)
- Drugs: Carvedilol, Metoprolol succinate, Bisoprolol
- Mechanism: ↓ sympathetic toxicity
- Dose (example):
* Carvedilol: 3.125 mg BD → 25 mg BD
- Contraindications: Acute decompensated HF, severe asthma
- Counseling: Do not stop abruptly
4. Mineralocorticoid Receptor Antagonists (MRA)
- Drugs: Spironolactone / Eplerenone
- Indication: NYHA II–IV, LVEF ≤35%
- Dose: 12.5–25 mg/day
- Adverse: Hyperkalemia, gynecomastia
- Monitoring: K⁺, renal function
5. SGLT2 Inhibitors
- Drugs: Dapagliflozin, Empagliflozin
- Indication: HFrEF with or without diabetes
- Dose: 10 mg once daily
- Benefits: ↓ mortality, ↓ hospitalization
- Adverse: Genital infections, dehydration
6. Diuretics (Symptomatic relief)
- Drug: Furosemide
- Dose: 20–80 mg/day (oral/IV)
- Mechanism: ↓ preload by natriuresis
- Adverse: Hypokalemia, hypotension
- Note: No mortality benefit, but essential
7. Other Drugs (Selected Patients)
- Ivabradine (sinus rhythm HR ≥70)
- Hydralazine + Isosorbide dinitrate
- Digoxin (AF with HF or persistent symptoms)
C. Management of HFpEF
- Control BP (ACEI/ARB)
- Diuretics for congestion
- Treat AF aggressively
- Manage comorbidities (DM, obesity, OSA)
D. Acute Decompensated Heart Failure
- Oxygen / NIV
- IV loop diuretics
- Vasodilators (nitroglycerin)
- Inotropes (dobutamine) if shock
- Treat precipitating cause
E. Device & Advanced Therapy
- ICD: LVEF ≤35% (sudden death prevention)
- CRT: Wide QRS with dyssynchrony
- LVAD
- Heart transplantation (end-stage HF)
10. Prognosis
- Depends on etiology, LVEF, NYHA class
- Improved significantly with guideline-directed medical therapy (GDMT)
11. Patient Counseling Points
- Adherence to medications is lifelong
- Daily weight monitoring (↑ >2 kg in 3 days → seek care)
- Recognize early symptoms of decompensation
- Avoid NSAIDs and excess salt
12. Key Exam & Clinical Pearls
- BNP normal → HF unlikely
- S3 = volume overload
- HFpEF common in elderly hypertensive women
- Four-pillar therapy saves lives in HFrEF