Percutaneous Coronary Intervention (PCI)
Definition
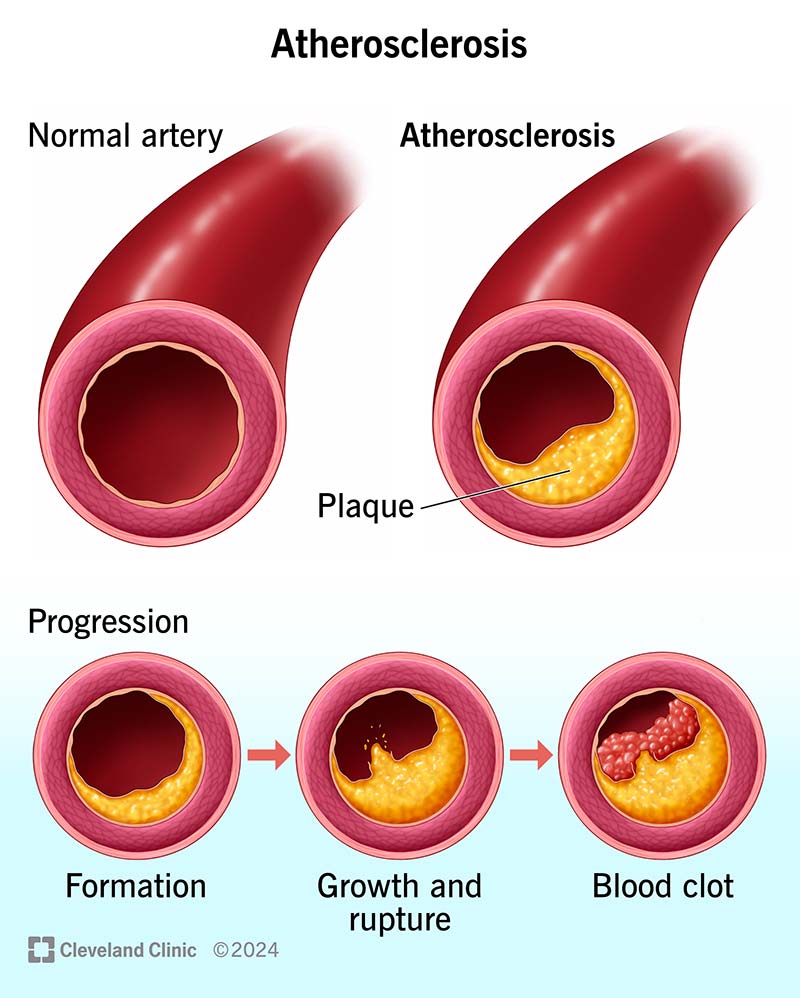
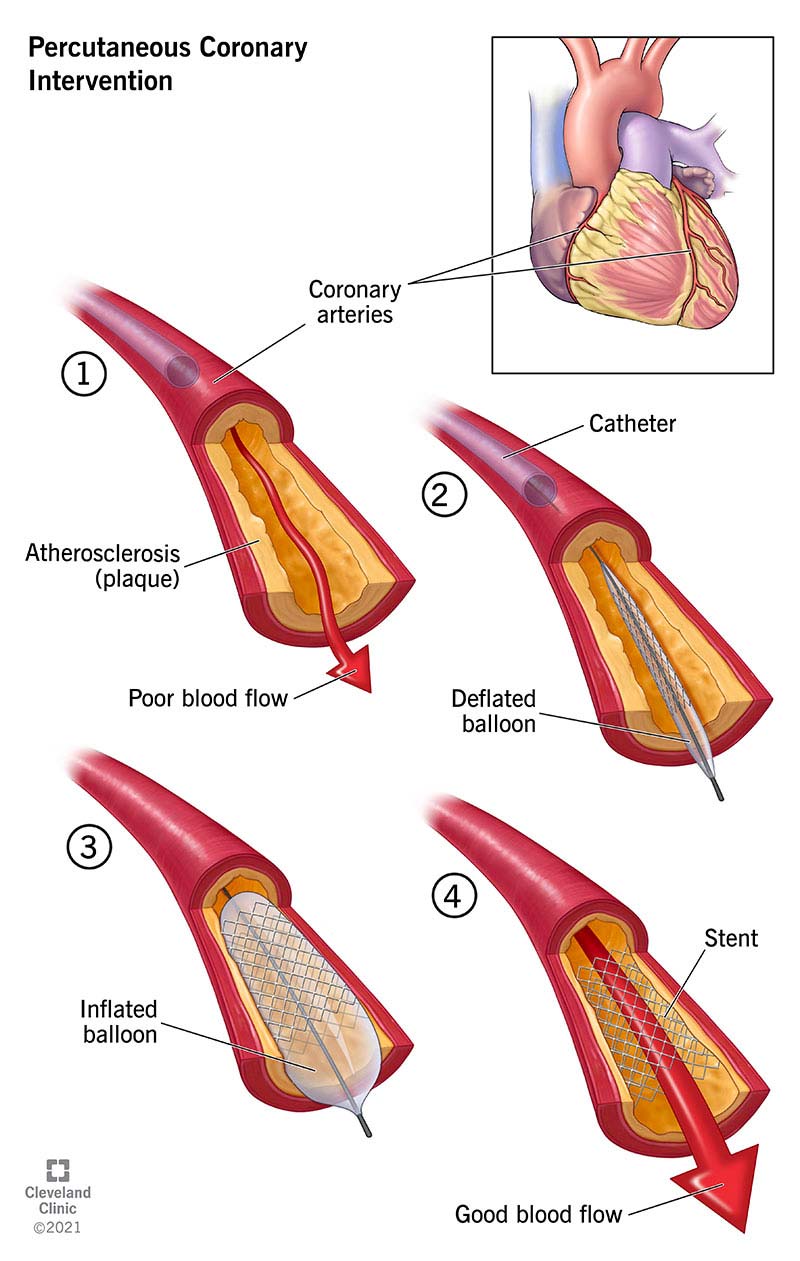
Percutaneous Coronary Intervention (PCI) is a minimally invasive, catheter-based procedure used to restore blood flow in stenosed or occluded coronary arteries by balloon dilatation and usually stent implantation. It is a cornerstone therapy for coronary artery disease (CAD) and acute coronary syndromes (ACS).
Indications
Acute Indications
- ST-Elevation Myocardial Infarction (STEMI) – primary PCI (gold standard)
- High-risk Non-STEMI / Unstable Angina
- Cardiogenic shock due to ischemia
- Ongoing ischemia despite optimal medical therapy
Elective / Chronic Indications
- Chronic stable angina with significant ischemia
- Prognostically significant lesions:
* Left main disease (selected cases)
* Proximal LAD disease
- Failed or contraindicated CABG in selected patients
Contraindications (Relative)
- Active bleeding or severe bleeding diathesis
- Severe contrast allergy (unless pre-treated)
- Advanced renal failure (relative)
- Diffuse disease unsuitable for PCI
- Poor vascular access
Coronary Anatomy Relevant to PCI
- Left Main Coronary Artery (LMCA)
- Left Anterior Descending (LAD)
- Left Circumflex (LCX)
- Right Coronary Artery (RCA)
Lesion complexity assessed by:
- SYNTAX score
- Lesion length, calcification, tortuosity
- Bifurcation involvement
- Chronic total occlusion (CTO)
Types of PCI
Based on Clinical Context
- Primary PCI – STEMI
- Rescue PCI – failed thrombolysis
- Elective PCI – stable CAD
- Staged PCI – multi-vessel disease
Based on Device
- Balloon angioplasty (POBA)
- Drug-Eluting Stents (DES) – standard of care
- Bare-Metal Stents (BMS) – rarely used
- Bioresorbable scaffolds (limited role)
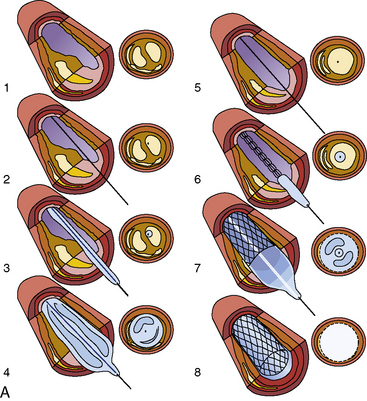
Step-by-Step PCI Procedure
- Vascular Access
* Radial artery (preferred)
* Femoral artery (complex cases)
- Diagnostic Coronary Angiography
* Defines lesion severity and anatomy
- Guide Catheter Placement
* Engages coronary ostium
- Guidewire Passage
* Crosses the lesion
- Lesion Preparation
* Balloon predilatation
* Cutting/scoring balloon
* Rotational atherectomy (calcified lesions)
- Stent Deployment
* DES inflated at high pressure
- Post-Dilatation
* Ensures optimal stent expansion
- Final Angiographic Assessment
* TIMI flow grade
* Residual stenosis
* Complications
Pharmacotherapy in PCI
Periprocedural Drugs
Antiplatelets
- Aspirin
* MOA: COX-1 inhibition → ↓ thromboxane A2
* Loading: 300 mg, Maintenance: 75–150 mg daily
- P2Y12 inhibitors
* Clopidogrel (300–600 mg load)
* Prasugrel
* Ticagrelor (preferred in ACS)
Anticoagulants
- Unfractionated Heparin
- Bivalirudin (selected cases)
GP IIb/IIIa inhibitors (selective use)
- Tirofiban, Eptifibatide
Post-PCI Medical Management
Dual Antiplatelet Therapy (DAPT)
- DES: minimum 12 months (ACS)
- Aspirin + P2Y12 inhibitor
Additional Therapy
- High-intensity statin
- Beta-blocker
- ACE inhibitor / ARB
- Lifestyle modification
Complications of PCI
Immediate
- Coronary dissection
- Acute stent thrombosis
- No-reflow phenomenon
- Arrhythmias
- Access-site bleeding
Early
- Contrast-induced nephropathy
- Subacute stent thrombosis
Late
- In-stent restenosis
- Late stent thrombosis
PCI vs CABG (Brief Comparison)
| Feature | PCI | CABG |
| -------------------- | ------------------ | --------------- |
| Invasiveness | Minimally invasive | Open surgery |
| Recovery | Faster | Slower |
| Multi-vessel disease | Limited | Superior |
| Diabetes | Inferior outcomes | Better outcomes |
| Repeat procedures | More common | Less common |
Outcomes & Prognosis
- Excellent symptom relief
- Reduces mortality in STEMI
- Outcome depends on:
* Timely reperfusion
* Complete revascularization
* Adherence to DAPT
Follow-Up After PCI
- Regular cardiology review
- Monitor for angina recurrence
- Lipid profile monitoring
- Blood pressure and glucose control
- Cardiac rehabilitation
Authoritative External References (Trusted)
- American College of Cardiology (ACC):
https://www.acc.org/tools-and-practice-support/clinical-topics/percutaneous-coronary-intervention
- European Society of Cardiology (ESC) Guidelines on PCI:
https://www.escardio.org/Guidelines/Clinical-Practice-Guidelines
- National Heart, Lung, and Blood Institute (NHLBI):
https://www.nhlbi.nih.gov/health/coronary-angioplasty
- Medscape PCI Overview:
https://emedicine.medscape.com/article/161446-overview
- UpToDate (Professional Reference):
https://www.uptodate.com/contents/percutaneous-coronary-intervention