Acute Respiratory Distress Syndrome (ARDS)
1. Definition
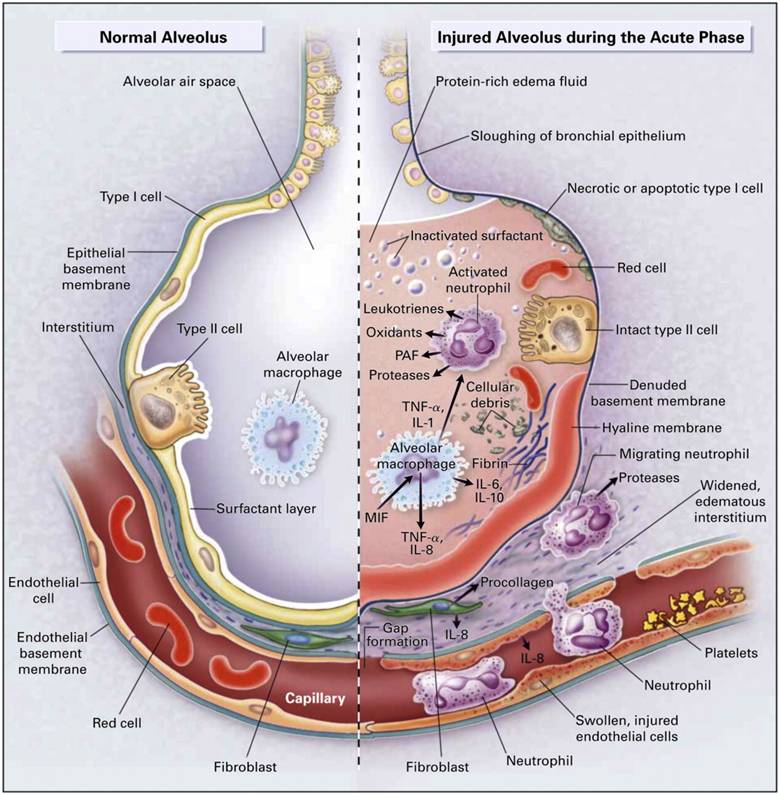
Acute Respiratory Distress Syndrome (ARDS) is a life-threatening form of acute hypoxemic respiratory failure caused by diffuse inflammatory injury to the alveolar–capillary membrane, leading to non-cardiogenic pulmonary edema, severe ventilation–perfusion mismatch, and refractory hypoxemia.
2. Epidemiology
- Common in ICU patients
- Mortality: 30–45% (higher with severe ARDS, older age, sepsis)
- Survivors may have long-term pulmonary and neuromuscular sequelae
3. Pathophysiology (Stepwise)
- Trigger (direct or indirect lung injury)
- Inflammatory cytokine release (TNF-α, IL-1, IL-6)
- Endothelial + epithelial damage
- ↑ Capillary permeability → protein-rich alveolar edema
- Surfactant dysfunction → alveolar collapse
- ↓ Lung compliance + ↑ shunt fraction
- Severe hypoxemia refractory to oxygen
Phases
| Phase | Features |
| ----------------------------- | ---------------------------------- |
| Exudative (Days 1–7) | Edema, hyaline membranes |
| Proliferative (Days 7–21) | Type II pneumocyte hyperplasia |
| Fibrotic (>3 weeks) | Pulmonary fibrosis (some patients) |
4. Etiology / Causes
Direct Lung Injury
- Pneumonia (bacterial, viral, COVID-19)
- Aspiration of gastric contents
- Inhalational injury (smoke, toxins)
- Pulmonary contusion
- Near drowning
Indirect Lung Injury
- Sepsis (most common)
- Severe trauma, shock
- Acute pancreatitis
- Massive blood transfusion (TRALI)
- Burns
- Drug overdose
5. Diagnostic Criteria (Berlin Definition)
All four must be present:
- Timing:
Within 1 week of known clinical insult
- Imaging:
Bilateral opacities on CXR/CT
(not fully explained by effusions, collapse, nodules)
- Origin of edema:
Respiratory failure not due to cardiac failure or fluid overload
(Echo or hemodynamics if doubt)
- Oxygenation (with PEEP ≥5 cm H₂O)
| Severity | PaO₂/FiO₂ |
| -------- | --------- |
| Mild | 200–300 |
| Moderate | 100–200 |
| Severe | <100 |
6. Clinical Features
Symptoms
- Acute onset severe dyspnea
- Tachypnea
- Refractory hypoxemia
- Restlessness, confusion
Signs
- Cyanosis
- Use of accessory muscles
- Diffuse crackles
- Hypotension (often with sepsis)
7. Investigations
Laboratory
- ABG: Hypoxemia ± respiratory alkalosis
- ↑ Lactate (if sepsis)
- CBC, CRP, procalcitonin (infection)
- Renal & liver function (MODS)
Imaging
- Chest X-ray: Bilateral diffuse infiltrates
- CT chest: Ground-glass opacities, consolidation
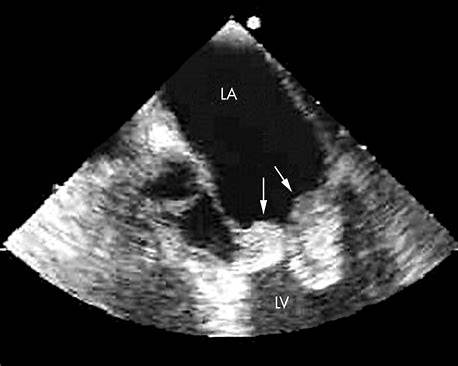
Cardiac Evaluation
- Echocardiography to exclude cardiogenic pulmonary edema
8. Differential Diagnosis
- Cardiogenic pulmonary edema
- Acute heart failure
- Pulmonary embolism
- Diffuse alveolar hemorrhage
- Acute interstitial pneumonia
- Pneumocystis pneumonia
9. Management (Cornerstone Section)
A. Treat Underlying Cause
- Early broad-spectrum antibiotics for sepsis
- Source control (drain abscess, stop transfusion)
- Treat pancreatitis, trauma, aspiration
B. Oxygenation & Ventilatory Support
1. Low Tidal Volume Ventilation (LTVV) – GOLD STANDARD
- Tidal volume: 6 mL/kg predicted body weight
- Plateau pressure: <30 cm H₂O
- Permissive hypercapnia allowed
2. PEEP Optimization
- Prevent alveolar collapse
- Moderate–high PEEP in moderate/severe ARDS
3. Prone Positioning
- Indicated when PaO₂/FiO₂ <150
- ≥ 16 hours/day
- Improves oxygenation and mortality
4. Neuromuscular Blockade
- Short course (≤48 h) in severe ARDS
- Improves ventilator synchrony
5. ECMO
- Refractory hypoxemia despite optimal ventilation
- Specialized centers only
C. Fluid Management
- Conservative fluid strategy
- Avoid positive fluid balance
- Diuretics once shock resolved
D. Pharmacologic Therapy
Corticosteroids
- Indication: Moderate–severe ARDS, especially early phase
- Benefit: ↓ ventilation days, possible mortality benefit
Example:
- Methylprednisolone 1–2 mg/kg/day (tapered)
⚠ Avoid late unregulated use
E. What is NOT Recommended
- Routine pulmonary artery catheter
- Routine nitric oxide
- Routine β-agonists
- High tidal volume ventilation
10. Drug Reference (Key Agents)
Sedatives (e.g., Propofol)
- Indication: Ventilator synchrony
- MOA: GABA-A agonist
- Adverse effects: Hypotension, hypertriglyceridemia
- Monitoring: BP, triglycerides
Neuromuscular Blockers (e.g., Cisatracurium)
- MOA: Non-depolarizing NMJ blockade
- Indication: Severe ARDS
- Adverse effects: Prolonged weakness
- Monitoring: TOF, ventilation
Antibiotics
- Based on suspected source
- Early empiric → de-escalate after cultures
11. Complications
- Ventilator-associated pneumonia
- Barotrauma (pneumothorax)
- Multi-organ dysfunction
- ICU-acquired weakness
- Pulmonary fibrosis
12. Prognosis
- Depends on:
* Severity (PaO₂/FiO₂)
* Age
* Cause (sepsis worse)
* Comorbidities
- Survivors may have:
* Reduced DLCO
* Exercise intolerance
* PTSD, cognitive dysfunction
13. Prevention
- Lung-protective ventilation in all ventilated patients
- Aspiration precautions
- Early sepsis management
- Judicious blood transfusion
14. Key Exam & Clinical Pearls
- ARDS = non-cardiogenic pulmonary edema
- Low tidal volume ventilation saves lives
- Prone positioning is underused but lifesaving
- Oxygen alone is often insufficient
- Always treat the underlying cause