Percutaneous Coronary Intervention (PCI)
Definition
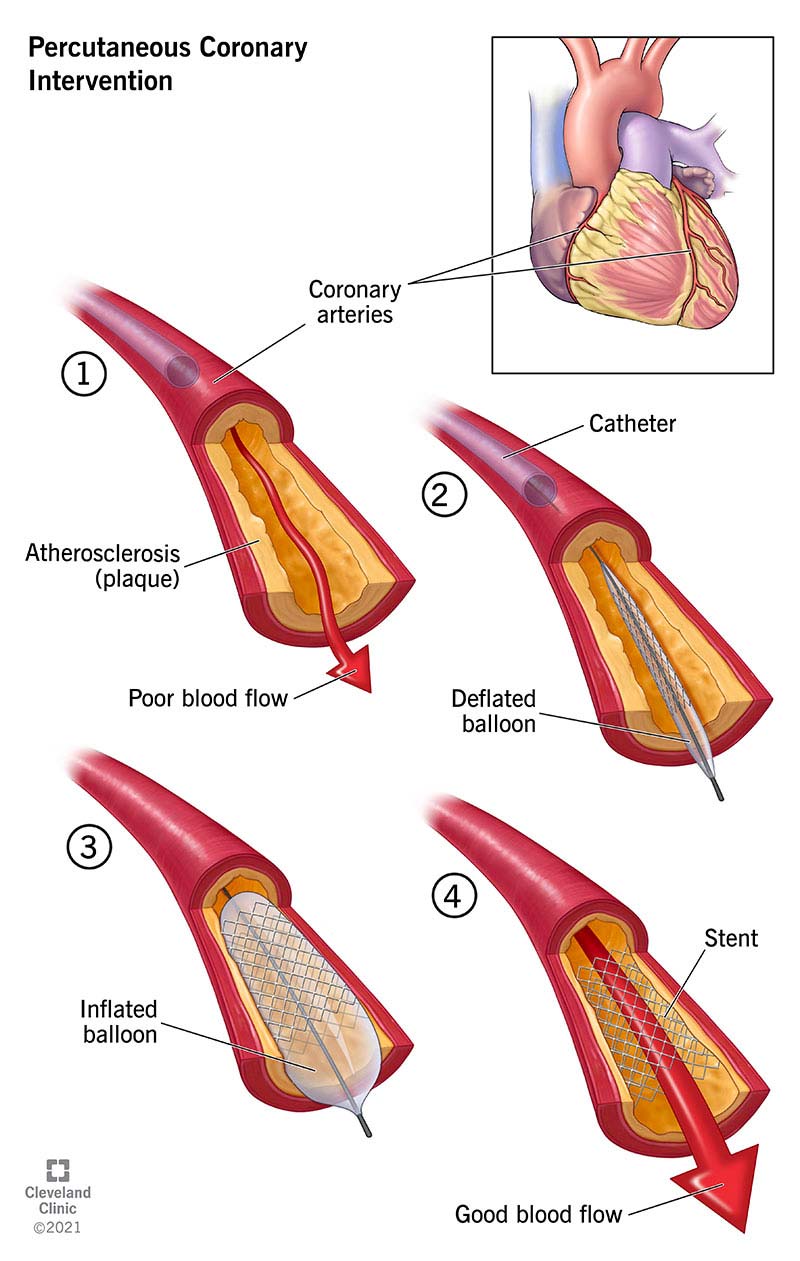
Percutaneous Coronary Intervention (PCI) is a minimally invasive, catheter-based procedure used to restore blood flow in narrowed or occluded coronary arteries due to atherosclerotic coronary artery disease. It is commonly called coronary angioplasty with or without stent placement.
Pathophysiology (Why PCI is needed)
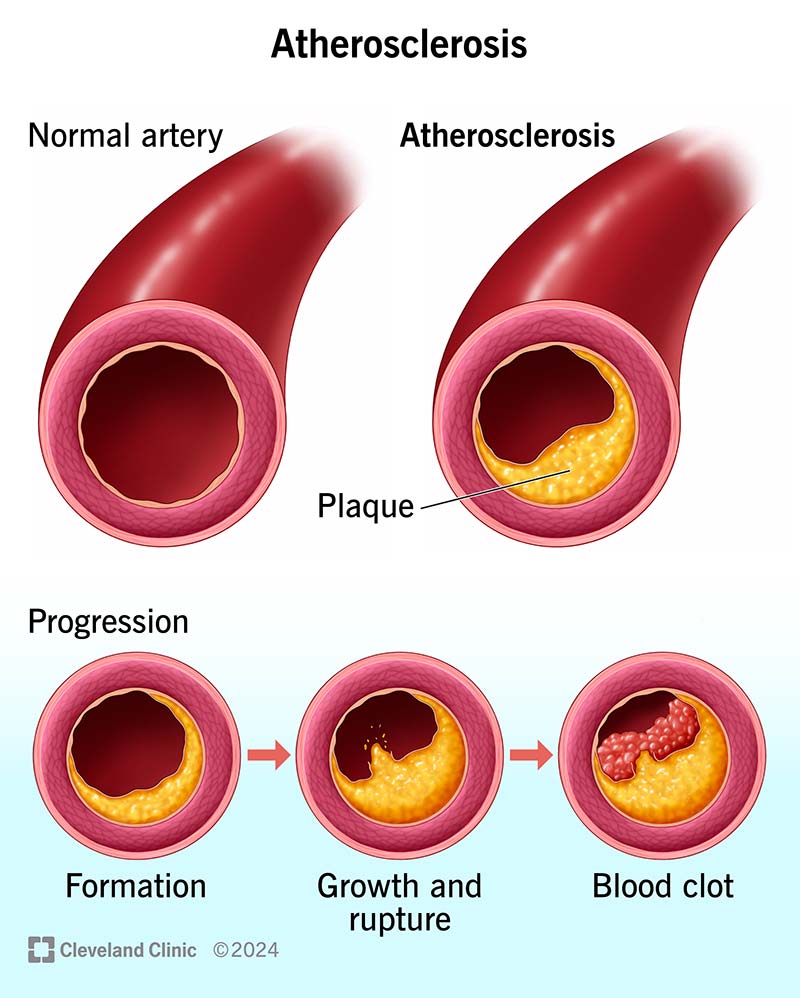
- Atherosclerosis → lipid-rich plaque forms in coronary arteries
- Progressive luminal narrowing → myocardial ischemia
- Plaque rupture → thrombus formation → acute coronary syndrome (ACS)
- PCI mechanically compresses plaque, dilates the artery, and often stabilizes the lesion with a stent
Indications
Absolute / Strong Indications
- ST-elevation myocardial infarction (STEMI) – primary PCI preferred
- High-risk NSTEMI / Unstable angina
- Refractory angina despite optimal medical therapy
- Hemodynamically significant coronary stenosis (>70%, or >50% left main)
Relative Indications
- Chronic stable angina with documented ischemia
- In-stent restenosis
- Cardiogenic shock due to coronary occlusion
Contraindications
Absolute
- Patient refusal
- No suitable vascular access (rare)
Relative
- Severe contrast allergy
- Advanced renal failure (risk of contrast nephropathy)
- Diffuse disease unsuitable for stenting
- Poor distal vessel runoff
Pre-Procedure Evaluation
- ECG – ischemia, infarction
- Cardiac biomarkers – troponin
- Coronary angiography – identifies lesion
- Echocardiography – LV function
- Renal function tests
- Coagulation profile
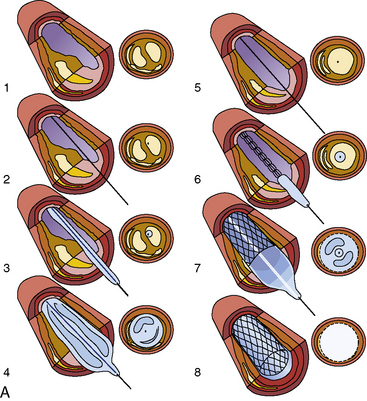
PCI Procedure (Stepwise)
- Vascular access – radial (preferred) or femoral artery
- Coronary angiography to localize lesion
- Guidewire passed across stenosis
- Balloon angioplasty (pre-dilatation)
- Stent deployment (DES or BMS)
- Post-dilatation & flow assessment (TIMI flow)
- Hemostasis & monitoring
Types of PCI
1. Balloon Angioplasty (PTCA)
- Rarely used alone due to recoil & restenosis
2. Stent PCI
- Bare Metal Stent (BMS) – higher restenosis
- Drug-Eluting Stent (DES) – releases antiproliferative drugs (preferred)
3. Special PCI Techniques
- Primary PCI – STEMI
- Rescue PCI – failed thrombolysis
- Elective PCI – stable CAD
- Complex PCI – bifurcation, CTO, left main
Drugs Used in PCI (Complete Reference)
1. Aspirin
- Indication: Antiplatelet backbone
- MOA: Irreversible COX-1 inhibition → ↓ TXA₂
- Dose:
* Loading: 150–325 mg
* Maintenance: 75–100 mg/day
- Adverse effects: GI bleeding, dyspepsia
- Contraindications: Active bleeding
- Monitoring: Bleeding signs
- Counselling: Lifelong unless contraindicated
2. P2Y12 Inhibitors (Dual Antiplatelet Therapy – DAPT)
a) Clopidogrel
- MOA: ADP receptor (P2Y12) inhibition
- Dose:
* Loading: 300–600 mg
* Maintenance: 75 mg/day
- Interactions: PPIs (omeprazole)
- Adverse effects: Bleeding, TTP (rare)
b) Ticagrelor
- Dose: 180 mg loading → 90 mg twice daily
- Advantages: Faster, reversible
- Adverse effects: Dyspnea, bradycardia
c) Prasugrel
- Contraindicated: Prior stroke/TIA, age >75
3. Anticoagulants
Unfractionated Heparin
- MOA: Activates antithrombin III
- Dose: 70–100 IU/kg IV
- Monitoring: ACT
- Risk: Bleeding, HIT
4. GP IIb/IIIa Inhibitors (Selective Use)
- Abciximab, Eptifibatide
- Used in high thrombus burden
Post-PCI Management
- DAPT duration:
* DES: ≥12 months (ACS), ≥6 months (stable CAD)
- Statins: High-intensity lifelong
- Beta blockers (if indicated)
- ACE inhibitors / ARBs
- Lifestyle modification (smoking cessation, diet, exercise)
Complications of PCI
Early
- Coronary dissection or perforation
- Acute stent thrombosis
- Arrhythmias
- Bleeding / hematoma
- Contrast-induced nephropathy
Late
- In-stent restenosis
- Late stent thrombosis
- Progression of native CAD
PCI vs CABG (Brief)
| Feature | PCI | CABG |
| ------------------------ | ------------------ | ------------ |
| Invasiveness | Minimally invasive | Open surgery |
| Recovery | Fast | Longer |
| Multivessel disease | Less effective | Preferred |
| Diabetes + triple vessel | Inferior | Superior |
Prognosis
- Excellent in STEMI when done early
- Symptom relief in stable CAD
- Survival benefit mainly in ACS, not routine stable angina