PANCREATIC NEUROENDOCRINE TUMOR (pNET)
1. Definition
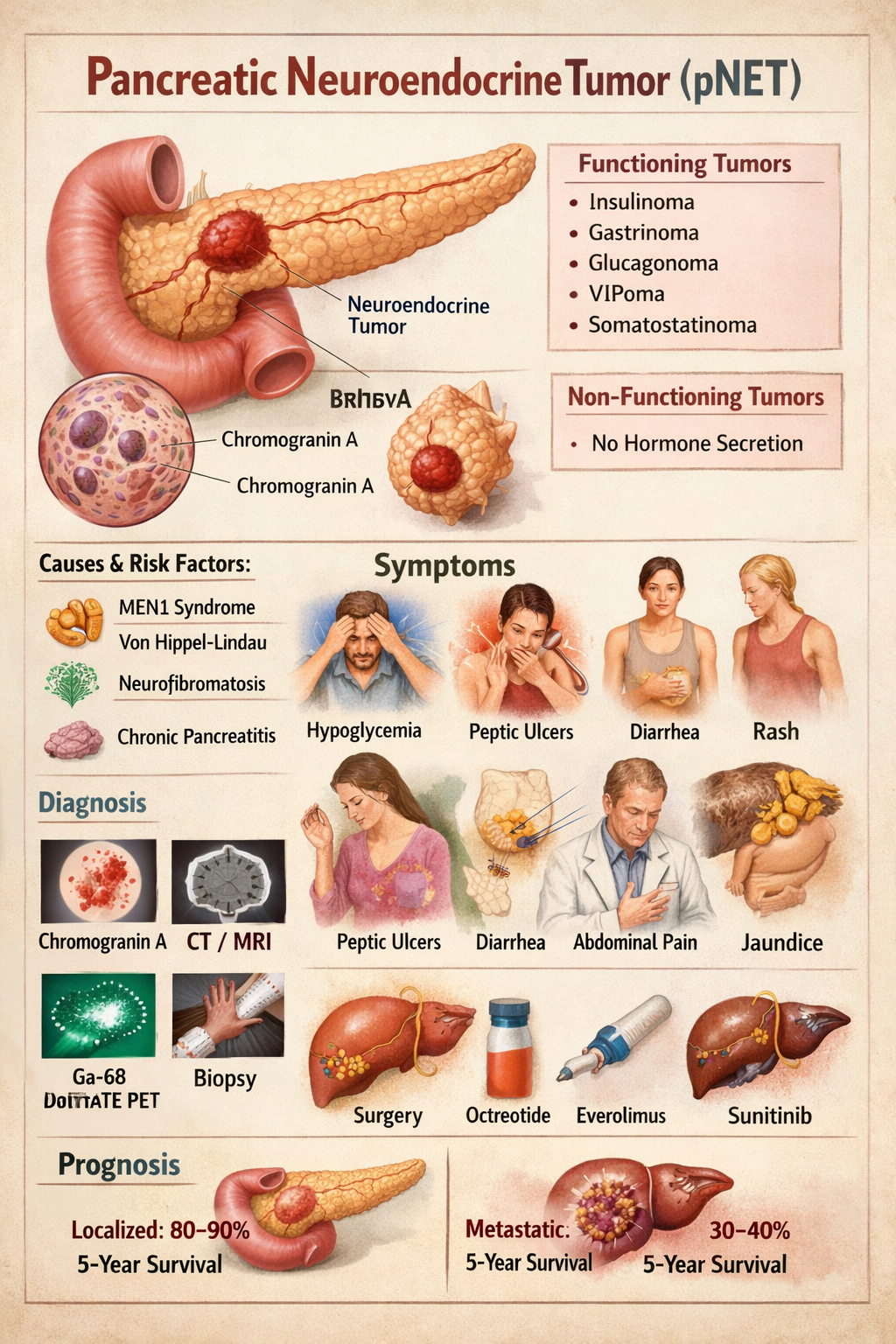
Pancreatic neuroendocrine tumors (pNETs) are neoplasms arising from endocrine (islet) cells of the pancreas that secrete peptide hormones or amines. They are biologically distinct from pancreatic adenocarcinoma and may be functioning (hormone-secreting) or non-functioning.
2. Pathophysiology
pNETs originate from enterochromaffin cells of pancreatic islets. They show:
- Neuroendocrine differentiation
- Dense-core secretory granules
- Expression of chromogranin A and synaptophysin
Tumor behavior depends on:
- Hormone secretion
- Tumor size
- Ki-67 index (mitotic rate)
- Invasion and metastasis
Tumors may be:
- Well differentiated (NET G1–G3)
- Poorly differentiated (Neuroendocrine carcinoma)
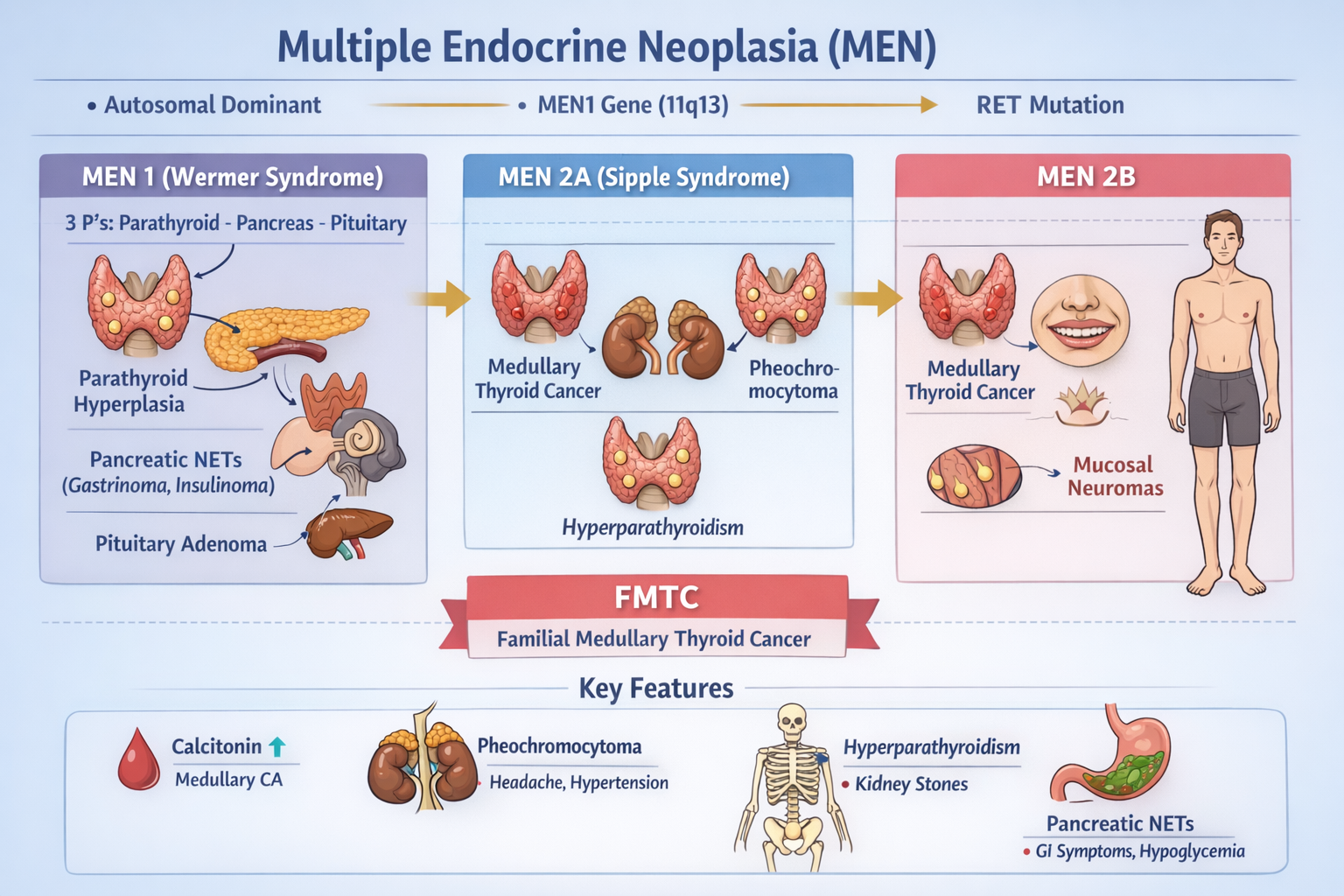
MEN1 mutation commonly involved → parathyroid, pituitary, pancreas tumors.
3. Classification
A. By hormone secretion
| Type | Hormone |
| --------------- | ------------ |
| Insulinoma | Insulin |
| Gastrinoma | Gastrin |
| Glucagonoma | Glucagon |
| VIPoma | VIP |
| Somatostatinoma | Somatostatin |
| Non-functioning | None |
B. By WHO grading
| Grade | Ki-67 |
| ----- | ----- |
| G1 | <3% |
| G2 | 3–20% |
| G3 | >20% |
4. Causes and Risk Factors
- MEN-1 syndrome
- Von Hippel–Lindau
- Neurofibromatosis-1
- Tuberous sclerosis
- Smoking
- Chronic pancreatitis
5. Clinical Features
A. Insulinoma
- Hypoglycemia
- Sweating
- Palpitations
- Confusion
- Weight gain
B. Gastrinoma (Zollinger-Ellison)
- Severe recurrent peptic ulcers
- Diarrhea
- GERD
C. Glucagonoma
- Diabetes
- Necrolytic migratory erythema
- Weight loss
- Anemia
D. VIPoma
- Profuse watery diarrhea
- Hypokalemia
- Achlorhydria
E. Somatostatinoma
- Diabetes
- Gallstones
- Steatorrhea
F. Non-functioning
- Abdominal pain
- Weight loss
- Jaundice
- Abdominal mass
- Metastasis symptoms
6. Investigations
Blood Tests
| Test | Use |
| ------------------ | --------------- |
| Chromogranin-A | Tumor marker |
| Insulin, C-peptide | Insulinoma |
| Gastrin | Gastrinoma |
| Glucagon | Glucagonoma |
| VIP | VIPoma |
| Somatostatin | Somatostatinoma |
| Fasting glucose | Hypoglycemia |
Imaging
- Contrast CT
- MRI pancreas
- Endoscopic ultrasound (best for small tumors)
- Ga-68 DOTATATE PET-CT (gold standard)
- Octreoscan
Biopsy
- EUS-guided biopsy
- Ki-67 index
7. Differential Diagnosis
- Pancreatic adenocarcinoma
- Islet cell hyperplasia
- Metastatic carcinoid
- Chronic pancreatitis
- Insulin autoimmune syndrome
8. Management
A. Curative – Surgery
- Enucleation (small insulinomas)
- Distal pancreatectomy
- Whipple procedure
- Liver metastasis resection
B. Medical Therapy
Used when metastatic, unresectable or hormone excess.
9. Drugs Used
1. Octreotide
Indication: Hormone control and tumor stabilization
Mechanism: Somatostatin analog → inhibits hormone secretion
Dose:
Adult: 100–500 mcg SC 2–3 times/day or 20–30 mg IM monthly
Paediatric: 1–10 mcg/kg/day
Adverse effects: Gallstones, diarrhea, hyperglycemia
Contraindication: Severe gallbladder disease
Monitoring: LFT, glucose
Counsel: May cause GI upset
2. Lanreotide
Same as octreotide
Dose: 120 mg SC every 4 weeks
3. Everolimus
Indication: Advanced pNET
Mechanism: mTOR inhibitor
Dose: 10 mg daily
Adverse: Mouth ulcers, hyperglycemia, infections
Contra: Active infection
Monitor: CBC, glucose
Counsel: Avoid live vaccines
4. Sunitinib
Indication: Metastatic pNET
Mechanism: VEGF receptor inhibitor
Dose: 37.5 mg daily
Adverse: Hypertension, fatigue
Contra: Cardiac failure
Monitor: BP, ECG
5. Diazoxide (for insulinoma)
Mechanism: Inhibits insulin release
Dose: 100–600 mg/day
Adverse: Fluid retention, hyperglycemia
Monitor: Glucose, edema
6. Streptozocin + 5-FU (Chemotherapy)
Indication: High-grade metastatic disease
Adverse: Nephrotoxicity, nausea
10. Non-Pharmacologic
- Surgical resection
- Radiofrequency ablation of liver mets
- Peptide receptor radionuclide therapy (PRRT)
- Dietary glucose support in insulinoma
11. Prognosis
- Localized pNET: 80–90% 5-year survival
- Metastatic: 30–40%
Better than pancreatic adenocarcinoma
12. Key Exam Points
- Insulinoma = most common pNET
- Gastrinoma = most malignant
- MEN1 = 3 P’s: Parathyroid, Pituitary, Pancreas
- Chromogranin A is universal tumor marker
- Ga-68 DOTATATE PET = best imaging