MULTIPLE ENDOCRINE NEOPLASIA (MEN)
1. Definition
Multiple Endocrine Neoplasia (MEN) is a group of inherited (autosomal dominant) tumor syndromes characterized by the development of two or more endocrine gland tumors in a single patient.
2. Types
| Type | Main Tumors |
| --------------------------- | ------------------------------------------------------------------------ |
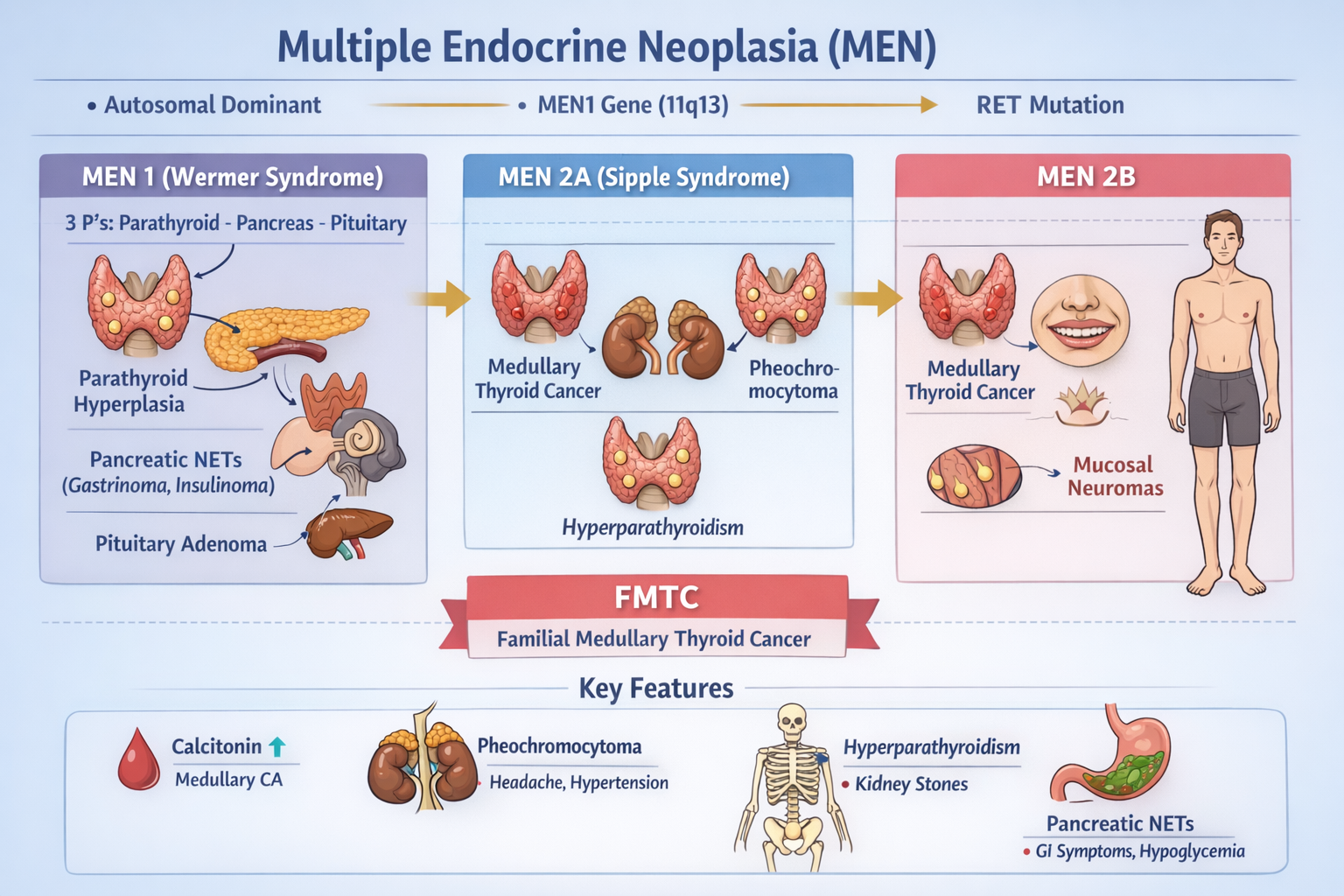
| MEN 1 (Wermer syndrome) | Parathyroid, Pancreatic NETs, Pituitary |
| MEN 2A | Medullary thyroid carcinoma (MTC), Pheochromocytoma, Hyperparathyroidism |
| MEN 2B | MTC, Pheochromocytoma, Mucosal neuromas, Marfanoid habitus |
| FMTC | Familial medullary thyroid carcinoma only |
MEN TYPE 1 (WERMMER SYNDROME)
3. Genetics & Pathophysiology
- Gene: MEN1 gene (11q13)
- Protein: Menin (tumor suppressor)
- Mechanism: Loss of tumor suppression → endocrine hyperplasia → tumors
Mnemonic: 3 P’s
> Parathyroid – Pancreas – Pituitary
4. Tumors in MEN 1
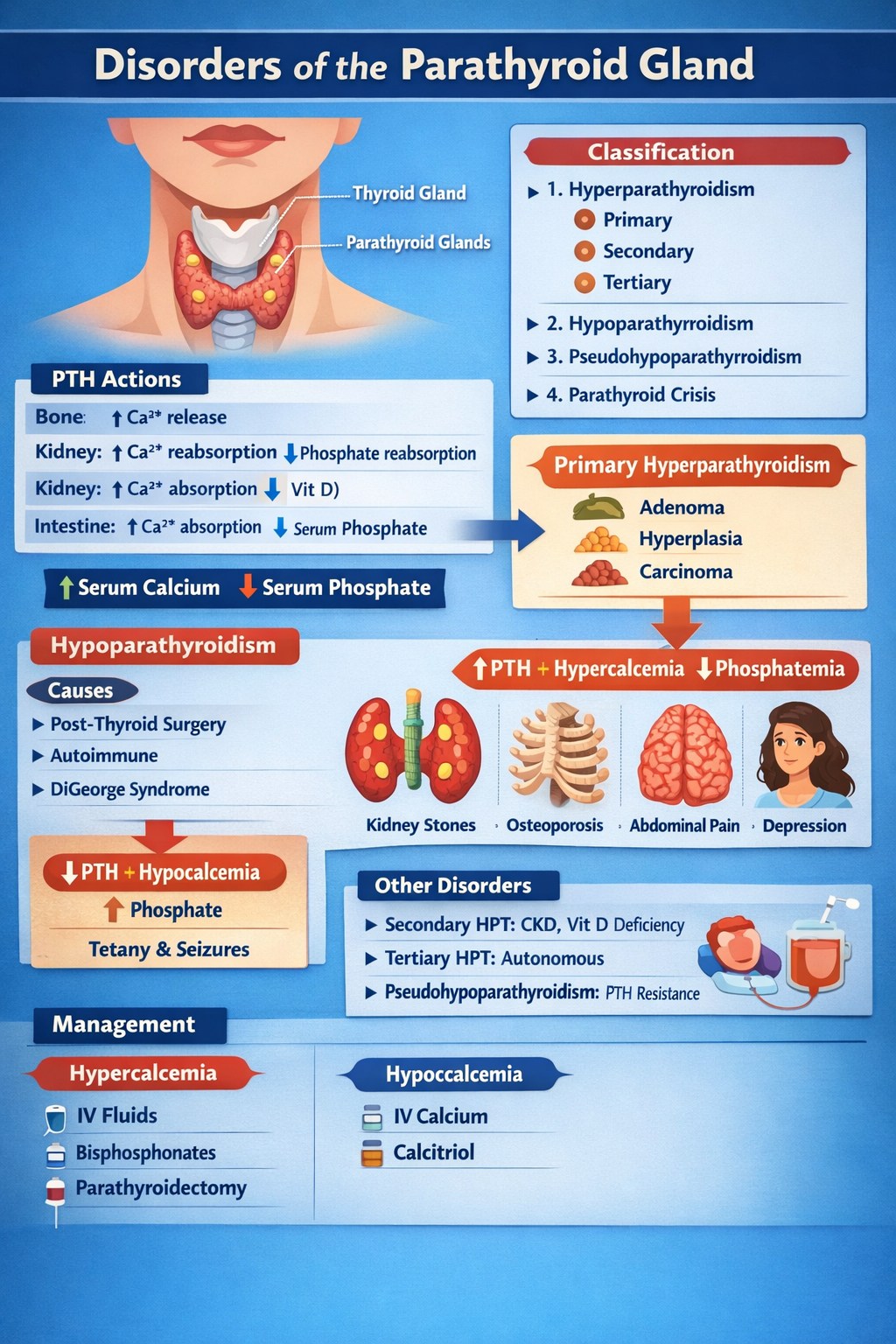
A. Primary Hyperparathyroidism (Most common)
- Seen in >90%
- Due to parathyroid hyperplasia
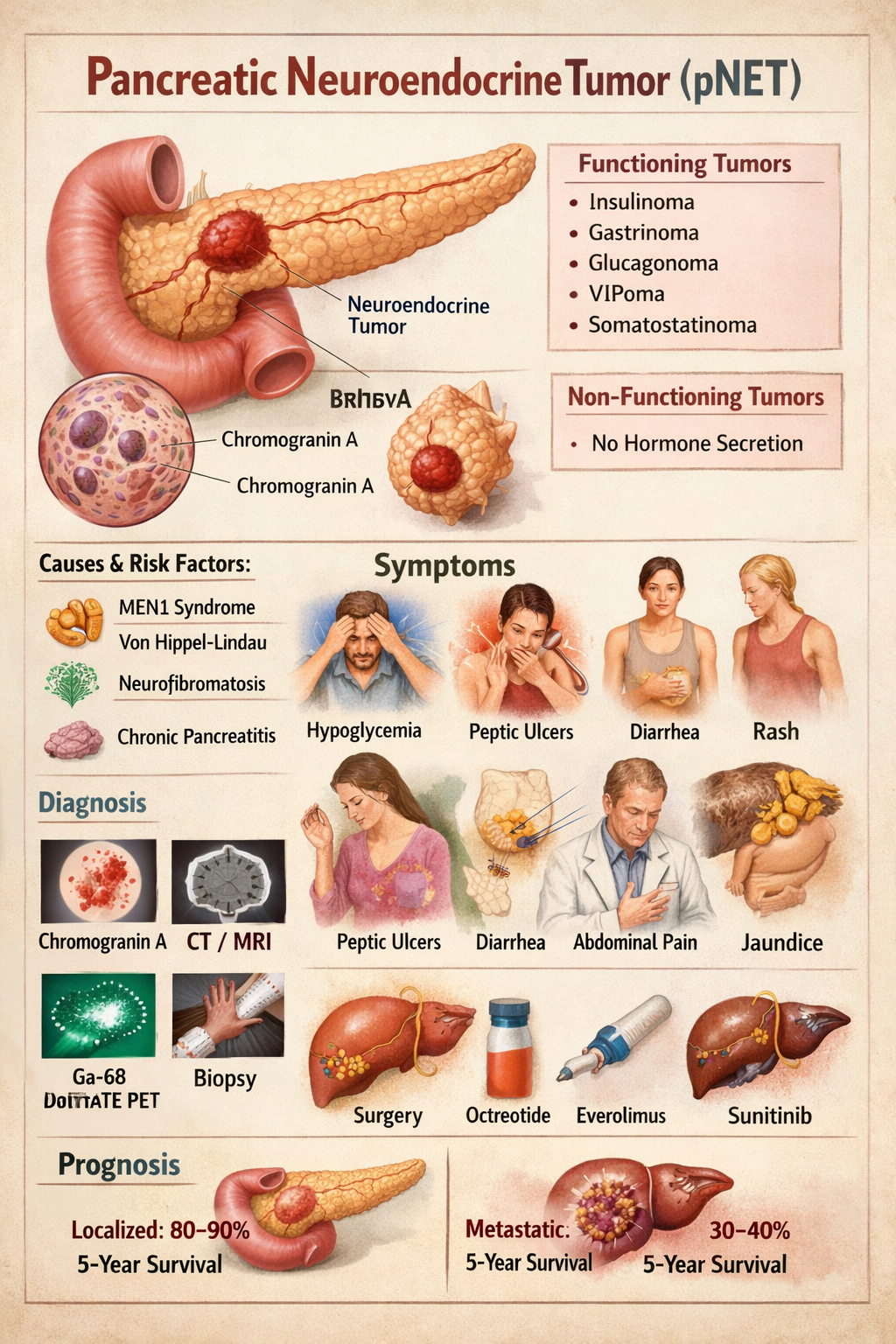
B. Pancreatic Neuroendocrine Tumors (NETs)
| Type | Hormone |
| --------------- | ------------ |
| Gastrinoma | Gastrin |
| Insulinoma | Insulin |
| Glucagonoma | Glucagon |
| VIPoma | VIP |
| Somatostatinoma | Somatostatin |
Most common = Gastrinoma
C. Pituitary Adenoma
- Prolactinoma (most common)
- GH, ACTH, non-functioning tumors
5. Clinical Features (MEN 1)
Hyperparathyroidism
- Bone pain, fractures
- Kidney stones
- Polyuria
- Depression
Gastrinoma (Zollinger–Ellison)
- Refractory peptic ulcers
- Diarrhea
- GI bleeding
Insulinoma
- Sweating
- Tremor
- Confusion
- Hypoglycemia relieved by glucose
Pituitary
- Galactorrhea
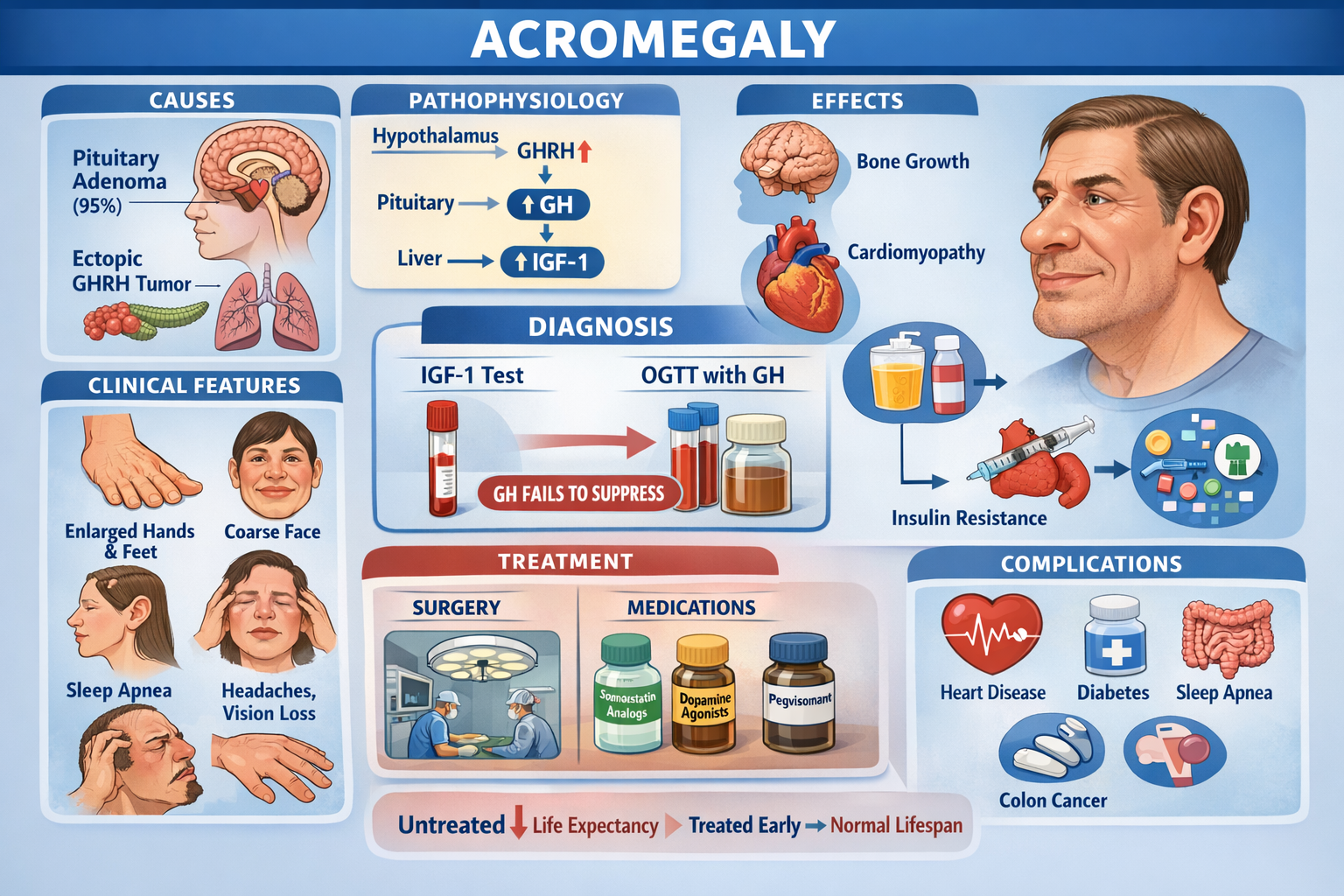
- Acromegaly
- Headache, visual loss
6. Investigations (MEN 1)
| Tumor | Tests |
| ------------ | -------------------------------- |
| Parathyroid | Serum Ca ↑, PTH ↑ |
| Gastrinoma | Fasting gastrin ↑, Secretin test |
| Insulinoma | Insulin, C-peptide, glucose |
| Pituitary | Prolactin, IGF-1, MRI |
| Localization | CT/MRI, EUS, PET-DOTATATE |
7. Management (MEN 1)
Parathyroid
- Subtotal parathyroidectomy
Pancreatic NET
- Surgical resection
- Somatostatin analogs for control
- PPIs for gastrinoma
Pituitary
- Dopamine agonists (prolactinoma)
- Surgery ± radiotherapy
MEN TYPE 2
Caused by RET proto-oncogene mutation
MEN 2A (Sipple Syndrome)
Tumors
- Medullary thyroid carcinoma (100%)
- Pheochromocytoma
- Hyperparathyroidism
Mnemonic: M P H
MEN 2B
Tumors
- Aggressive medullary thyroid carcinoma
- Pheochromocytoma
- Mucosal neuromas
- Marfanoid body
8. Medullary Thyroid Carcinoma (MTC)
Pathophysiology
- From C-cells
- Secretes Calcitonin
Features
- Thyroid nodule
- Diarrhea
- Flushing
- Neck lymphadenopathy
9. Pheochromocytoma
Pathophysiology
- Tumor of adrenal medulla → catecholamine excess
Features
- Episodic headache
- Sweating
- Palpitations
- Hypertension
10. Investigations (MEN 2)
| Tumor | Test |
| ---------------- | --------------------- |
| MTC | Serum calcitonin, CEA |
| Pheochromocytoma | Plasma metanephrines |
| Parathyroid | Calcium, PTH |
| Genetics | RET mutation testing |
11. Treatment (MEN 2)
Order of Surgery (Very important)
> Pheochromocytoma → Thyroid → Parathyroid
Because removing thyroid before pheo can cause fatal hypertensive crisis.
Thyroid
- Total thyroidectomy
- Prophylactic in RET-positive children
Pheochromocytoma
- Alpha-blocker → beta-blocker → surgery
12. Prophylactic Thyroidectomy
| RET mutation | Age |
| ------------ | ----------- |
| MEN 2B | At birth |
| MEN 2A | By 5 years |
| FMTC | By 10 years |
13. Key Differences
| Feature | MEN 1 | MEN 2 |
| ------------------- | ------ | ---------- |
| Gene | MEN1 | RET |
| MTC | No | Yes |
| Hyperparathyroidism | Common | Mild in 2A |
| Pancreatic NET | Yes | No |
| Pheochromocytoma | No | Yes |
14. High-yield Exam Points
- MEN1 = 3 Ps
- MEN2A = MTC + Pheo + HPT
- MEN2B = MTC + Pheo + Neuromas
- Always treat pheochromocytoma before thyroid
- Calcitonin = tumor marker for MTC