CUSHING SYNDROME – COMPLETE CLINICAL REFERENCE
1. Definition
Cushing syndrome is the clinical state resulting from chronic exposure to excess glucocorticoids, either exogenous (iatrogenic) or endogenous (ACTH-dependent or ACTH-independent), leading to characteristic metabolic, cardiovascular, musculoskeletal, dermatologic, and neuropsychiatric abnormalities.
> Cushing disease = ACTH-secreting pituitary adenoma (subset of Cushing syndrome)
2. Pathophysiology
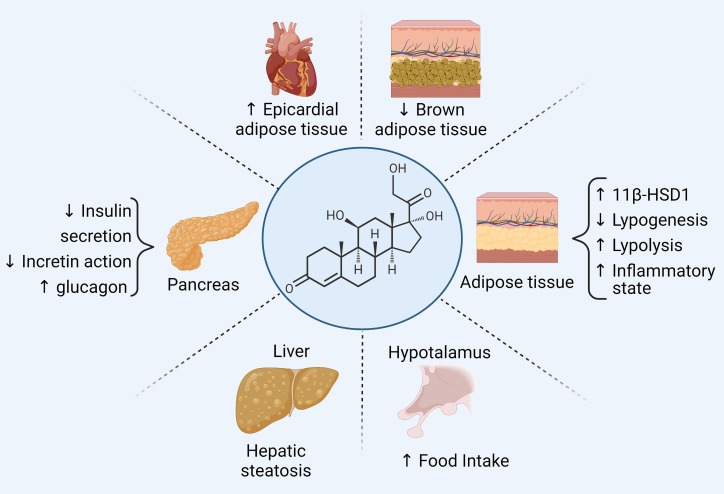
Excess cortisol causes:
- Protein catabolism → muscle wasting, thin skin, osteoporosis
- Increased gluconeogenesis + insulin resistance → diabetes
- Lipolysis with fat redistribution → central obesity, moon face, buffalo hump
- Mineralocorticoid receptor activation (at high cortisol levels) → hypertension, hypokalemia
- Immunosuppression → infections
- Suppression of HPG axis → hypogonadism, infertility
- Neurotransmitter imbalance → depression, psychosis, cognitive decline
3. Etiology / Causes
A. Exogenous (Most common)
- Chronic glucocorticoid therapy (oral, inhaled, topical, injectable)
B. Endogenous
1. ACTH-Dependent (≈70%)
- Pituitary adenoma (Cushing disease)
- Ectopic ACTH secretion
* Small cell lung carcinoma
* Bronchial carcinoid
* Thymic tumors
* Pancreatic neuroendocrine tumors
2. ACTH-Independent (≈30%)
- Adrenal adenoma
- Adrenal carcinoma
- Macronodular adrenal hyperplasia
- Micronodular adrenal hyperplasia (PPNAD)
4. Clinical Features
General
- Central (truncal) obesity
- Moon facies
- Buffalo hump
- Weight gain with thin extremities
Skin
- Purple striae (>1 cm, abdomen/thighs)
- Easy bruising
- Thin skin
- Acne
- Poor wound healing
- Hirsutism (women)
Musculoskeletal
- Proximal muscle weakness (hips, shoulders)
- Osteoporosis
- Vertebral fractures
- Growth retardation (children)
Metabolic
- Diabetes mellitus
- Dyslipidemia
- Weight gain
Cardiovascular
- Hypertension
- Accelerated atherosclerosis
- Increased cardiovascular mortality
Neuropsychiatric
- Depression
- Irritability
- Anxiety
- Psychosis
- Cognitive impairment
- Sleep disturbance
Reproductive
- Amenorrhea / oligomenorrhea
- Infertility
- Decreased libido
- Erectile dysfunction
Immune
- Recurrent infections
- Opportunistic infections
5. Investigations / Diagnosis
Step 1: Confirm Hypercortisolism (Any ONE positive)
- Overnight 1 mg dexamethasone suppression test
* Normal: cortisol < 1.8 µg/dL
* Cushing: failure to suppress
- 24-hour urinary free cortisol (UFC)
* Elevated (>3× upper limit)
- Late-night salivary cortisol
* Elevated (loss of diurnal rhythm)
> At least two abnormal tests recommended
Step 2: Determine ACTH Dependence
- Plasma ACTH
* Low → ACTH-independent (adrenal)
* Normal/high → ACTH-dependent
Step 3: Localize Source
ACTH-Dependent
- High-dose dexamethasone suppression test
* Suppression → pituitary
* No suppression → ectopic
- CRH stimulation test
- MRI pituitary
- Inferior petrosal sinus sampling (gold standard)
ACTH-Independent
- CT / MRI adrenal glands
6. Differential Diagnosis
- Pseudo-Cushing states:
* Depression
* Alcoholism
* Obesity
* Poorly controlled diabetes
- Polycystic ovary syndrome
- Metabolic syndrome
- Hypothyroidism
7. Management (Stepwise)
A. Exogenous Cushing
- Gradual tapering of steroids
- Never abrupt withdrawal (risk of adrenal crisis)
B. Endogenous Cushing
1. Surgical (Definitive)
- Transsphenoidal surgery (pituitary adenoma)
- Adrenalectomy (adrenal tumors)
- Resection of ectopic ACTH tumor
2. Medical Therapy (Pre-op / Inoperable / Persistent disease)
a. Steroidogenesis Inhibitors
Ketoconazole
- Indication: Hypercortisolism control
- MOA: Inhibits adrenal CYP enzymes
- Dose: 200–400 mg 2–3×/day
- Adverse effects: Hepatotoxicity, gynecomastia
- Monitoring: LFTs
- Contraindications: Liver disease
- Interactions: CYP3A4 inhibition
- Counselling: Report jaundice, fatigue
Metyrapone
- MOA: Inhibits 11-β-hydroxylase
- Dose: 250 mg 3–4×/day
- Adverse effects: Hypertension, hirsutism
- Monitoring: BP, electrolytes
Osilodrostat
- MOA: Potent 11-β-hydroxylase inhibitor
- Adverse effects: Adrenal insufficiency, QT prolongation
b. Pituitary-Directed Therapy
Cabergoline
- MOA: Dopamine D2 agonist
- Indication: Mild Cushing disease
- Adverse effects: Nausea, orthostasis
Pasireotide
- MOA: Somatostatin analog
- Adverse effects: Hyperglycemia
- Monitoring: Blood glucose
c. Glucocorticoid Receptor Antagonist
Mifepristone
- Indication: Cushing with diabetes
- MOA: Blocks cortisol receptor
- Adverse effects: Hypokalemia, endometrial thickening
- Monitoring: Clinical response (cortisol not reliable)
3. Radiotherapy
- For residual or recurrent pituitary disease
8. Complications
- Cardiovascular disease (leading cause of death)
- Diabetes complications
- Osteoporotic fractures
- Severe infections
- Adrenal insufficiency after treatment
9. Special Situations
Pregnancy
- Prefer surgery in 2nd trimester
- Avoid most medical therapies
Children
- Growth failure prominent
- Higher suspicion required
10. Prognosis
- Untreated: High morbidity and mortality
- Treated: Gradual recovery over months–years
- Persistent metabolic risk even after cure
11. Key Exam Pearls
- Most common cause: Exogenous steroids
- Most common endogenous cause: Pituitary adenoma
- Gold standard localization: Inferior petrosal sinus sampling
- Purple striae >1 cm → highly suggestive
- Hypokalemic alkalosis → ectopic ACTH