Normal Growth in Pediatrics — Detailed Guide
1. What Is Growth?
Growth in children refers to the increase in body size and mass over time. It reflects nutritional status, health, endocrine function, genetics, and overall development.
Key measurable growth parameters:
- Weight
- Height/length
- Head circumference
- Body mass index (BMI)
- Growth velocity (rate of change over time)
2. Growth Measurement Techniques
Weight
- Infants (<2 years): Measured naked using calibrated infant scales.
- Older children: Standard upright scale, light clothing, no shoes.
- Recording: In kilograms (kg) or grams (g).
Length / Height
- Infants (<24 months): Recumbent length using infantometer.
- Older children (>24 months): Standing height using stadiometer.
- Recording: In centimeters (cm) to one decimal.
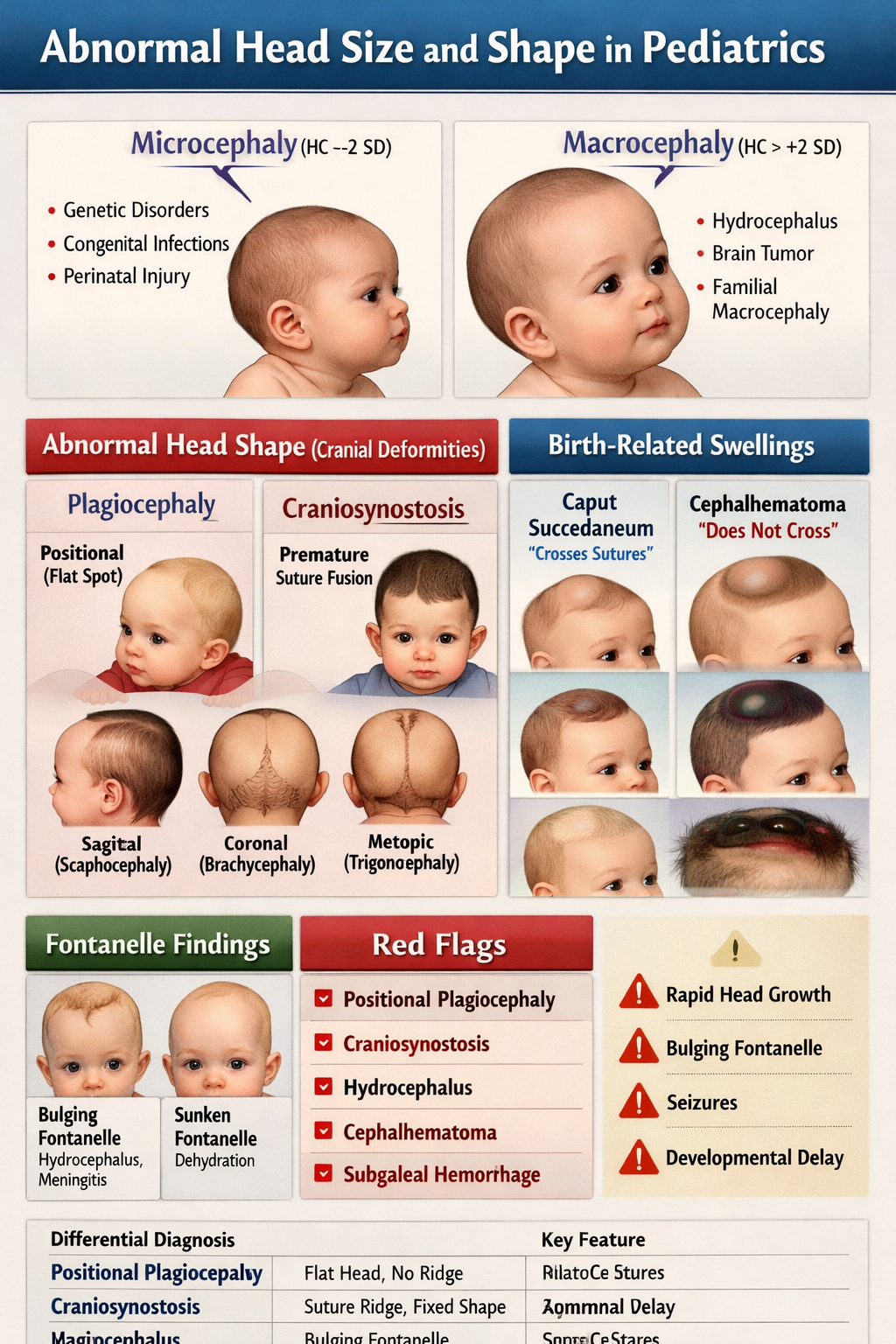
Head Circumference
- Around the largest part of the head above eyebrows and occiput.
- Important in infants <3 years to assess brain growth.
- Recording: In cm.
BMI
- BMI = weight (kg) / height (m)^2
- Used to assess underweight, overweight, obesity in children >2 years.
3. Growth Patterns by Age
A. Infancy (0–12 months)
- Birth weight: Normal term neonate ~2.8–3.5 kg.
- First 5–7 days: Expected slight weight loss (5–10%), regained by 10–14 days.
- 0–6 months: ~150–200 g/week weight gain.
- By 4–6 months: Birth weight doubles.
- By 12 months: Birth weight triples.
- Length/height: ~25 cm increase in first year.
- Head circumference: ~12 cm increase in first year.
B. Toddler (1–3 years)
- Weight gain slows to ~2–3 kg/year.
- Height increases ~10–12 cm/year.
- Head circumference growth slows.
C. Early Childhood (3–5 years)
- Steady growth: ~2–3 kg/year and ~6–7 cm/year.
- Proportionate body changes.
D. Middle Childhood (6–10 years)
- Consistent linear growth ~5–6 cm/year and ~2–3 kg/year.
- Prepubertal period with steady pacing.
E. Puberty (Girls ~8–13, Boys ~9–14)
- Growth spurt:
* Girls: Peak ~10–12 years.
* Boys: Peak ~12–14 years.
- Very rapid height velocity: up to ~8–10 cm/year.
- Weight increases with muscle/fat distribution changes.
- Complete by ~16–18 years (girls earlier than boys).
4. Growth Velocity
The rate of growth (e.g., cm/year, kg/year).
- Infants and toddlers have the highest velocities.
- Decelerates in early childhood.
- Peaks again in puberty.
- Important for early detection of growth disorders.
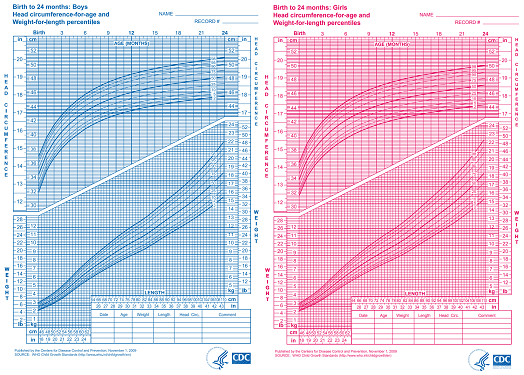
5. Growth Standards and Percentiles
Growth Charts
Children are plotted on standardized growth charts to assess if they are:
- Normal
- Above average
- Below average
Common charts:
- WHO growth standards (birth to 5 years)
- CDC growth charts (2–20 years)
- Country-specific references
Percentiles
- 5th–85th percentile: Generally considered normal.
- <3rd percentile: Suggests possible undergrowth.
- >97th percentile: Suggests possible overgrowth or obesity.
6. Body Proportions in Growth
- Infants: Legs shorter proportionally; head larger relative to body.
- Adolescents: Legs grow faster then torso, body proportions balance out.
7. Factors Influencing Growth
A. Genetic
- Parental heights determine target height range.
- Mid-parental height formula:
* Boys = (father + mother + 13 cm)/2
* Girls = (father + mother − 13 cm)/2
B. Nutrition
- A critical driver in infancy and early childhood.
- Malnutrition → poor weight gain and stunting.
C. Hormonal
- Growth hormone
- Thyroid hormone
- Sex steroids (in puberty)
D. Systemic Illness
- Chronic conditions (renal, cardiac, GI diseases) slow growth.
E. Psychosocial
- Environmental, emotional neglect can impair growth (“psychosocial dwarfism”).
8. Clinical Interpretation of Growth Data
Look at:
- Current plotted percentile
- Growth curve pattern over time
- Growth velocity
- Target height range
- Proportion and body ratios
- Head circumference trend (especially in infants)
Sudden drops in percentile or crossing percentiles downward is concerning.
9. Common Abnormal Growth Patterns
A. Failure to Thrive (FTT)
- Weight drops below expected trend.
- Causes: inadequate intake, malabsorption, chronic diseases.
B. Stunting
- Low height-for-age.
- Often chronic malnutrition or systemic disease.
C. Wasting
- Low weight-for-height.
- Acute weight loss or severe malnutrition.
D. Obesity
- High BMI-for-age.
- Risk of metabolic syndrome.
10. When to Be Concerned
Growth should be evaluated if:
- Weight or height drops >2 major percentiles.
- Growth velocity slows over time.
- Extreme percentiles persist without familial support.
- Abnormal body proportions.
- Developmental delays accompany growth issues.
11. Key Takeaways
- Growth reflects overall health; precise measurements over time are essential.
- Normal growth follows predictable age-specific patterns.
- Interpretation requires serial plotting, not a single measurement.
- Early detection of abnormal patterns allows timely intervention.