Abnormality of Head Size and Shape in Pediatrics (Detailed)
Head size and shape abnormalities are very common concerns in pediatrics and may reflect benign variation or serious neurologic/skeletal pathology.
1. Normal Head Growth Basics
Head Circumference (HC)
- Reflects brain growth
- Measured using a non-stretchable tape around:
* Forehead (supraorbital ridge)
* Occipital prominence
Normal Growth Rate
- 0–3 months: ~2 cm/month
- 3–6 months: ~1 cm/month
- 6–12 months: ~0.5 cm/month
- 1–3 years: ~1 cm/year
- After 3 years: very slow growth
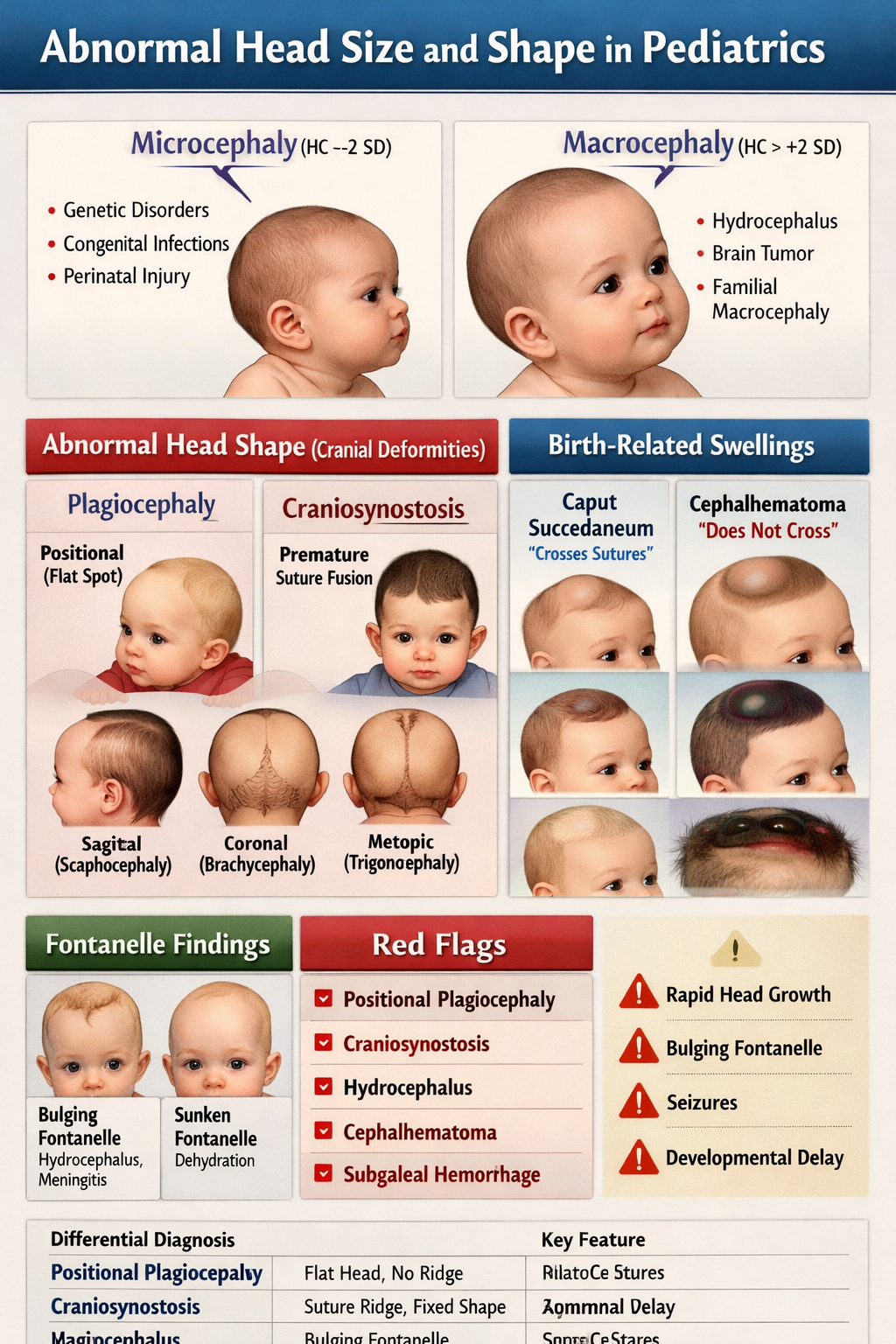
2. Abnormal Head Size
A. Microcephaly
Definition
- HC < –2 SD below mean
- Severe: < –3 SD
Pathophysiology
- Reduced brain volume due to:
* Poor neuronal proliferation
* Early brain injury
* Genetic syndromes
Causes
Congenital
- Chromosomal disorders (Trisomy 13, 18)
- Genetic syndromes (Rett, Angelman)
- Congenital infections (TORCH)
* CMV, Rubella, Toxoplasmosis, Zika
Acquired
- Hypoxic ischemic injury
- Severe malnutrition
- Metabolic disorders (PKU)
Clinical Features
- Small head size
- Developmental delay
- Seizures
- Spasticity
- Dysmorphic features
Investigations
- MRI brain
- TORCH screening
- Genetic testing
- Metabolic screening
Management
- Treat underlying cause
- Early developmental therapy
- Seizure control if needed
B. Macrocephaly
Definition
- HC > +2 SD above mean
- Severe: > +3 SD
Pathophysiology
- Increased intracranial volume due to:
* Enlarged brain
* Excess CSF
* Blood/space-occupying lesion
Causes
Benign
- Familial macrocephaly
- Benign enlargement of subarachnoid spaces (BESS)
Pathologic
- Hydrocephalus
- Intracranial tumor
- Subdural hematoma (abuse)
- Storage disorders (Tay-Sachs)
Clinical Features
- Enlarged head
- Bulging fontanelle
- Vomiting
- Irritability
- Sunset eye sign (hydrocephalus)
- Developmental delay
Investigations
- Cranial ultrasound (infants)
- MRI brain
- CT if emergency
Management
- Hydrocephalus → VP shunt or endoscopic third ventriculostomy
- Treat underlying pathology
3. Abnormal Head Shape (Cranial Deformities)
A. Plagiocephaly
Definition
- Asymmetrical flattening of skull
Types
- Positional plagiocephaly (benign)
- Synostotic plagiocephaly (craniosynostosis)
Causes
- Sleeping position (back-to-sleep)
- Torticollis
- Prematurity
Clinical Features
- Flattening of occiput
- Ear shifted forward on affected side
- No ridging of sutures
Management
- Repositioning therapy
- Physiotherapy for torticollis
- Helmet therapy (severe, 4–12 months)
B. Craniosynostosis
Definition
Premature fusion of cranial sutures → abnormal skull shape + restricted brain growth.
Types & Shapes
| Suture fused | Shape |
| -------------------- | ------------------------------------ |
| Sagittal | Scaphocephaly (long narrow skull) |
| Coronal (one side) | Anterior plagiocephaly |
| Coronal (both sides) | Brachycephaly (short broad skull) |
| Metopic | Trigonocephaly (triangular forehead) |
| Lambdoid | Posterior plagiocephaly |
Clinical Features
- Abnormal head shape from birth
- Palpable ridge over fused suture
- Increased ICP signs:
* Vomiting
* Papilledema
* Developmental delay
Investigations
- Skull X-ray (suture closure)
- CT 3D reconstruction (gold standard)
Management
- Surgical correction ideally before 1 year
- Monitor neurodevelopment
C. Caput Succedaneum
Definition
- Scalp edema above periosteum
Features
- Present at birth
- Crosses suture lines
- Resolves in 1–2 days
Management
- Reassurance only
D. Cephalhematoma
Definition
- Subperiosteal hemorrhage
Features
- Does NOT cross sutures
- Appears hours after birth
- Risk of jaundice
Management
- Observe
- Treat hyperbilirubinemia if needed
E. Subgaleal Hemorrhage (Emergency)
Definition
Bleeding between scalp aponeurosis and periosteum.
Cause
- Vacuum-assisted delivery
Clinical Features
- Diffuse boggy swelling
- Crosses sutures widely
- Shock, pallor, tachycardia
Management
- NICU admission
- Volume resuscitation
- Blood transfusion if needed
4. Abnormal Fontanelle Findings
Bulging Fontanelle
Causes
- Meningitis
- Hydrocephalus
- Intracranial hemorrhage
Action
- Emergency evaluation
Sunken Fontanelle
Cause
- Dehydration
Management
- Rehydration
Delayed Closure
Causes
- Hypothyroidism
- Rickets
- Down syndrome
- Raised ICP
5. Differential Diagnosis Summary
| Condition | Key Feature |
| ------------------------ | -------------------------------------- |
| Positional plagiocephaly | No suture ridging |
| Craniosynostosis | Ridge + fixed deformity |
| Hydrocephalus | Rapid HC increase + bulging fontanelle |
| Cephalhematoma | Does not cross sutures |
| Caput succedaneum | Crosses sutures, resolves fast |
| Subgaleal hemorrhage | Shock + diffuse swelling |
6. Red Flags (Urgent Referral)
- Rapid head circumference increase
- Bulging fontanelle
- Developmental regression
- Seizures
- Persistent vomiting
- Suspected craniosynostosis
- Signs of abuse (subdural bleed)
7. Key Takeaway
Abnormal head size and shape in pediatrics may represent:
- Normal variants (familial macrocephaly, positional plagiocephaly)
- Serious neurologic disorders (hydrocephalus, craniosynostosis, genetic syndromes)
- Birth-related swellings (caput, cephalhematoma, subgaleal hemorrhage)
Early recognition and appropriate imaging/referral are critical.