Abnormalities of Stature in Pediatrics
1. Definition
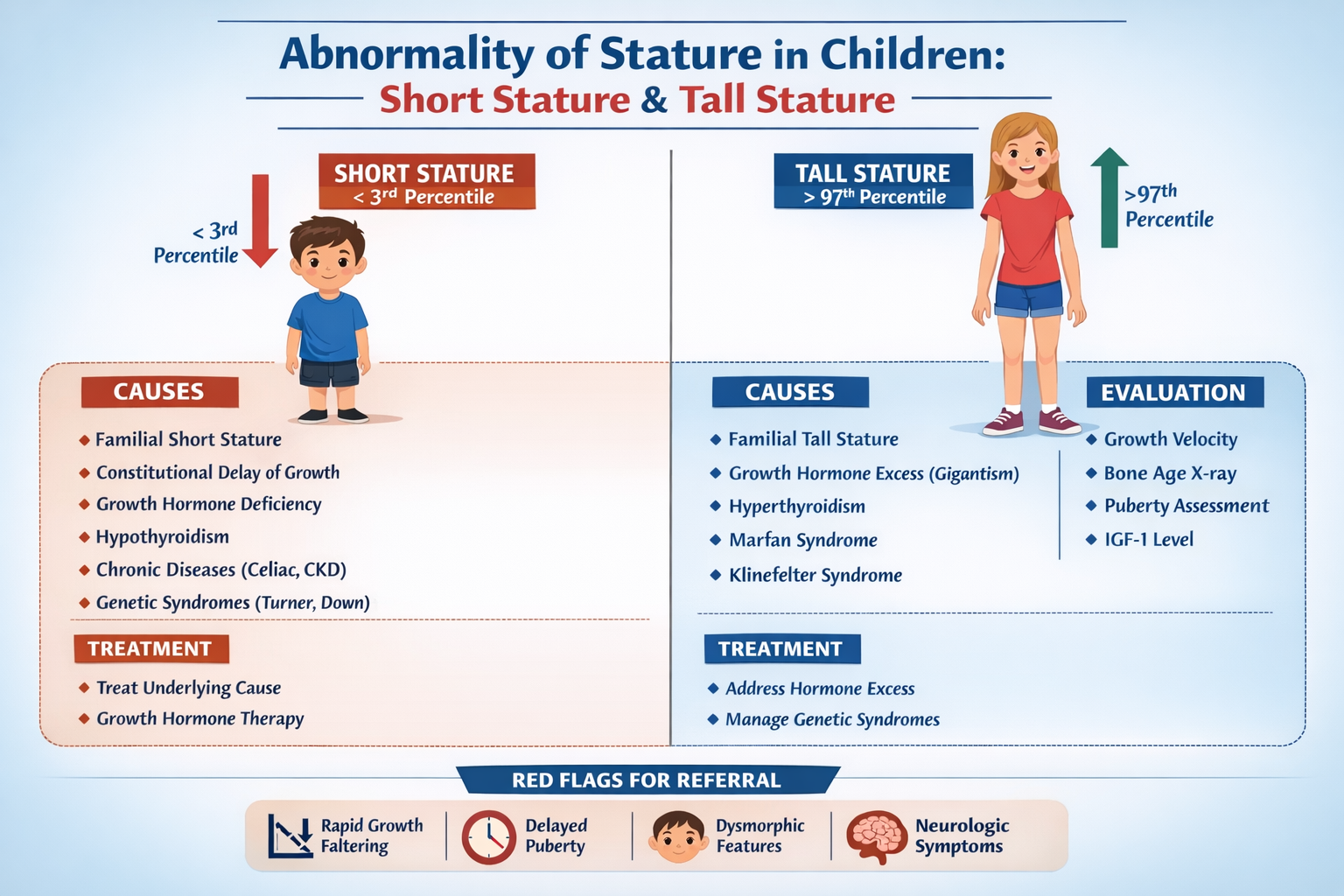
Abnormal stature refers to a child's height significantly below or above the expected range for age and sex.
It is usually defined as:
- Short stature: Height < −2 SD (below 3rd percentile) on standard growth charts.
- Tall stature: Height > +2 SD (above 97th percentile) for age and sex.
Assessment must consider:
- Age
- Sex
- Genetic potential (mid-parental height)
- Growth velocity
Short Stature
Definition
Height below the 3rd percentile or < −2 standard deviations for age and sex.
Important Concepts
- Growth velocity: Normally 5–7 cm/year after age 2
- Disproportionate vs proportionate short stature
Causes of Short Stature
1. Normal Variants
These are most common causes.
Familial Short Stature
- Short parents
- Normal growth velocity
- Bone age = chronological age
- Final height appropriate for family
Constitutional Growth Delay
- Delayed puberty
- Delayed bone age
- Normal adult height eventually
- Family history of late growth
2. Endocrine Causes
Growth failure due to hormone deficiency.
Growth Hormone Deficiency
Features:
- Proportionate short stature
- Delayed bone age
- Increased fat mass
- Immature face
- Delayed dentition
Causes:
- Congenital pituitary defect
- Pituitary tumors
- Cranial irradiation
Hypothyroidism
Features:
- Short stature
- Weight gain
- Delayed bone age
- Dry skin
- Constipation
- Slow growth velocity
Cushing Syndrome
- Growth failure
- Obesity
- Moon face
- Hypertension
3. Chronic Systemic Diseases
Chronic illness affects nutrition and metabolism.
Examples:
- Chronic kidney disease
- Congenital heart disease
- Malabsorption
- Chronic infections
- Inflammatory bowel disease
Mechanisms:
- Poor nutrition
- Hormonal disturbance
- Chronic inflammation
4. Genetic and Chromosomal Disorders
Turner Syndrome (Girls)
Features:
- Short stature
- Webbed neck
- Shield chest
- Gonadal dysgenesis
- Lymphedema at birth
Down Syndrome
- Mild short stature
- Characteristic facial features
Skeletal Dysplasias
Example:
- Achondroplasia
Features:
- Disproportionate short stature
- Short limbs
- Normal trunk
5. Nutritional Causes
Most common worldwide.
Examples:
- Protein energy malnutrition
- Micronutrient deficiencies
- Chronic undernutrition
6. Psychosocial Causes
Psychosocial dwarfism
Features:
- Emotional deprivation
- Growth hormone suppression
- Poor weight gain
- Improves after environmental change
Tall Stature
Definition
Height above 97th percentile or > +2 SD for age.
Causes of Tall Stature
1. Familial Tall Stature
- Tall parents
- Normal growth velocity
- Normal bone age
- Normal puberty
2. Endocrine Causes
Growth Hormone Excess
- Gigantism (before epiphyseal closure)
- Rapid growth
- Large hands and feet
Causes:
- Pituitary adenoma
Hyperthyroidism
Features:
- Accelerated growth
- Weight loss
- Tachycardia
- Heat intolerance
Precocious Puberty
- Early puberty
- Early growth spurt
- Early epiphyseal closure
- Final height may be reduced
3. Genetic Syndromes
Marfan Syndrome
Features:
- Tall stature
- Long limbs
- Arachnodactyly
- Lens dislocation
- Aortic dilation
Klinefelter Syndrome
Features:
- Tall males
- Long legs
- Hypogonadism
- Gynecomastia
Sotos Syndrome
- Cerebral gigantism
- Macrocephaly
- Developmental delay
Evaluation of Abnormal Stature
1. History
Important points:
- Birth weight and length
- Nutritional history
- Chronic illness
- Drug history (steroids)
- Puberty timing
- Family height
2. Physical Examination
Measurements:
- Height
- Weight
- Head circumference
- Body proportions
Look for:
- Dysmorphic features
- Skeletal abnormalities
- Pubertal staging (Tanner stage)
3. Growth Chart Analysis
Plot height on:
- WHO growth charts
- Serial measurements
Assess:
- Percentile crossing
- Growth velocity
4. Mid-Parental Height
For boys:
[
\text{Father height + Mother height + 13} / 2
]
For girls:
[
\text{Father height + Mother height − 13} / 2
]
Expected adult height range:
± 8.5 cm
5. Bone Age Assessment
Method:
- X-ray left wrist
Interpretation:
- Bone age = chronological age → familial
- Bone age delayed → endocrine causes
- Bone age advanced → precocious puberty
6. Laboratory Investigations
Basic Tests
- CBC
- ESR
- Renal function
- Liver function
- Thyroid function
Hormonal Tests
- IGF-1
- Growth hormone stimulation test
Genetic Testing
- Karyotype (Turner syndrome)
Management
Normal Variants
- Reassurance
- Growth monitoring
Endocrine Disorders
Treat underlying disease.
Examples:
Growth Hormone Therapy
Drug: Recombinant Growth Hormone
Indications:
- GH deficiency
- Turner syndrome
- Chronic renal failure
- Small for gestational age
Dose:
- 0.025–0.035 mg/kg/day SC
Adverse Effects:
- Intracranial hypertension
- Slipped capital femoral epiphysis
- Edema
- Insulin resistance
Monitoring:
- Growth velocity
- IGF-1 levels
- Thyroid function
Nutritional Causes
- Nutritional rehabilitation
- Micronutrient supplementation
Genetic Disorders
- Multidisciplinary management
- Genetic counseling
Red Flag Signs (Pathological Short Stature)
Refer urgently if:
- Height < −3 SD
- Growth velocity < 4 cm/year
- Dysmorphic features
- Delayed puberty
- Chronic illness signs
- Disproportionate body segments
✅ Summary
| Condition | Key Feature |
| ---------------------- | --------------------------------- |
| Familial short stature | Short parents, normal bone age |
| Constitutional delay | Delayed puberty, delayed bone age |
| GH deficiency | Delayed bone age + poor growth |
| Hypothyroidism | Short + weight gain |
| Turner syndrome | Short girl + webbed neck |
| Achondroplasia | Disproportionate short stature |
| Marfan syndrome | Tall + long limbs |
| Gigantism | GH excess |
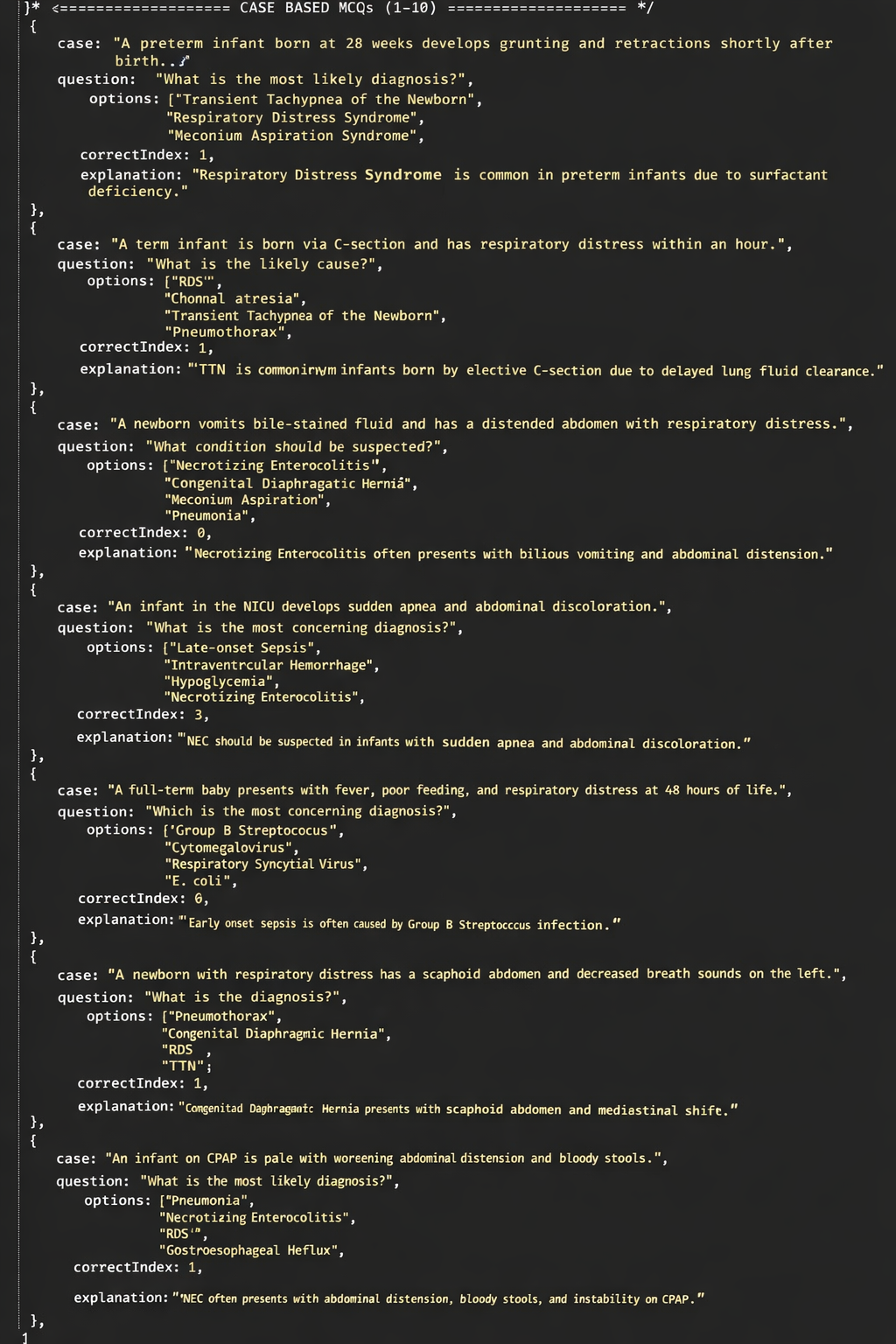
If you want, I can also give 30 pediatric MCQs on abnormalities of stature (very useful for NEET-PG / FMGE / NEXT preparation).