Abnormalities of Head Size and Shape in Pediatrics
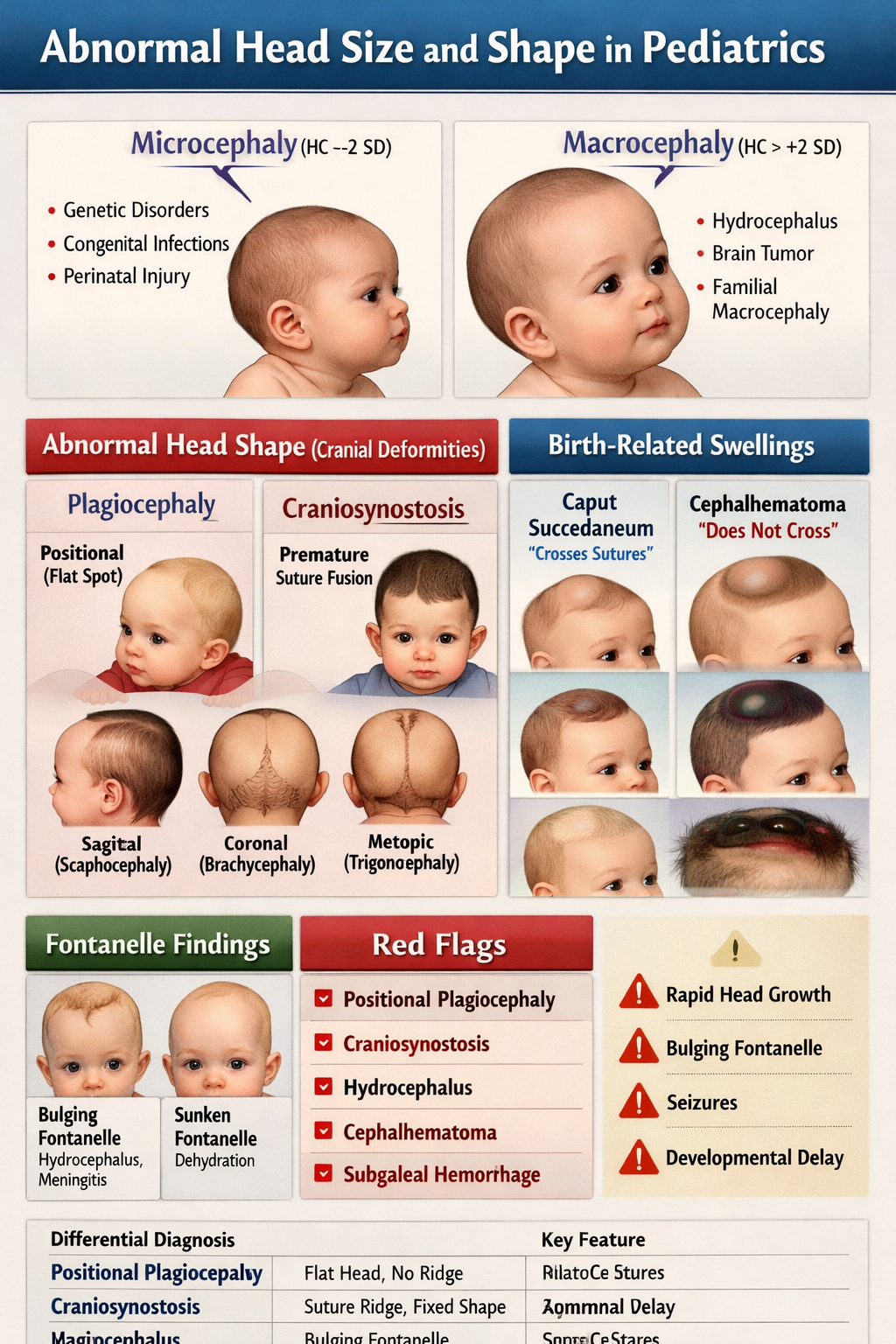
Abnormal head size and shape in children can indicate underlying neurological, genetic, developmental, or structural disorders. Assessment is primarily based on head circumference (HC), cranial shape, sutures, and fontanelles.
1. Abnormal Head Size
A. Microcephaly
Definition
Microcephaly is a condition where the head circumference is significantly smaller than normal for age and sex, usually < −2 SD (standard deviations) below the mean or <3rd percentile.
Pathophysiology
- Reduced brain growth leads to reduced skull growth.
- Skull bones grow according to brain expansion; therefore impaired neuronal development results in a small skull.
Causes
Primary (genetic)
- Autosomal recessive primary microcephaly
- Chromosomal abnormalities
Secondary causes
- Intrauterine infections (TORCH infections)
- Maternal alcohol exposure
- Severe malnutrition
- Perinatal hypoxic injury
- Metabolic disorders
- Radiation exposure
Clinical Features
- Small head circumference
- Sloping forehead
- Developmental delay
- Intellectual disability
- Seizures
- Spasticity or cerebral palsy
- Feeding difficulties
- Visual or hearing problems
Investigations
- Serial head circumference measurements
- Neuroimaging (MRI preferred)
- TORCH screening
- Genetic testing
- Metabolic screening
Differential Diagnosis
- Craniosynostosis
- Intrauterine growth restriction
- Skeletal dysplasia
Management
No definitive cure. Treatment is supportive and rehabilitative.
Management approach
- Early developmental therapy
- Physiotherapy
- Occupational therapy
- Speech therapy
- Management of seizures
Drug for seizures:
Medication: Phenobarbital
Indication
Neonatal seizures
Mechanism
Enhances GABA-mediated inhibition in CNS.
Dose
- Neonate loading: 20 mg/kg IV
- Maintenance: 3–5 mg/kg/day
Adverse effects
- Sedation
- Respiratory depression
- Cognitive impairment
Monitoring
- Serum levels
- Respiratory status
Prognosis
Depends on severity and underlying cause.
B. Macrocephaly
Definition
Macrocephaly is head circumference > +2 SD above the mean (>97th percentile) for age and sex.
Pathophysiology
Enlargement of the head due to:
- Increased brain size
- Increased cerebrospinal fluid
- Skull thickening
- Mass lesions
Causes
Benign causes
- Familial macrocephaly
- Benign enlargement of subarachnoid space
Pathological causes
- Hydrocephalus
- Intracranial tumors
- Storage disorders
- Neurocutaneous syndromes
- Subdural hematoma
Clinical Features
- Large head
- Bulging anterior fontanelle
- Dilated scalp veins
- Sunset sign (downward eye deviation)
- Vomiting
- Irritability
- Developmental delay
Investigations
- Serial head circumference charting
- Cranial ultrasound (infants)
- CT scan
- MRI brain
- Genetic evaluation if syndromic
Differential Diagnosis
- Hydrocephalus
- Megalencephaly
- Craniosynostosis
Management
Treatment depends on cause.
Example: Hydrocephalus treatment
- Ventriculoperitoneal shunt surgery
- Endoscopic third ventriculostomy
Prognosis
Varies widely based on etiology.
2. Abnormal Head Shape
A. Craniosynostosis
Definition
Premature fusion of one or more cranial sutures, resulting in abnormal skull growth.
Pathophysiology
- Skull growth occurs perpendicular to sutures.
- Premature suture fusion restricts growth in one direction and causes compensatory expansion in others.
Types
| Type | Suture Involved | Skull Shape |
| -------------- | ------------------ | ------------------- |
| Scaphocephaly | Sagittal | Long narrow head |
| Brachycephaly | Coronal bilateral | Short wide head |
| Plagiocephaly | Unilateral coronal | Asymmetric skull |
| Trigonocephaly | Metopic | Triangular forehead |
Causes
- Isolated craniosynostosis
- Genetic syndromes
* Apert syndrome
* Crouzon syndrome
* Pfeiffer syndrome
Clinical Features
- Abnormal skull shape
- Palpable ridge along fused suture
- Early closure of fontanelle
- Increased intracranial pressure
- Developmental delay
Investigations
- Skull X-ray
- CT scan with 3D reconstruction
- Genetic testing
Management
- Surgical correction
- Cranial remodeling surgery
- Helmet therapy (in mild cases)
Prognosis
Good if treated early.
B. Positional Plagiocephaly
Definition
Flattening of one side of the head due to external pressure, commonly from sleeping position.
Causes
- Supine sleeping
- Torticollis
- Prematurity
- Limited neck movement
Clinical Features
- Flattened occiput
- Asymmetric head shape
- Ear displacement
Investigations
Mostly clinical diagnosis.
Management
- Repositioning therapy
- Tummy time
- Physiotherapy
- Helmet therapy (severe cases)
Prognosis
Usually resolves with growth.
3. Other Cranial Shape Abnormalities
| Condition | Description |
| -------------- | ------------------ |
| Dolichocephaly | Long narrow head |
| Brachycephaly | Short broad skull |
| Plagiocephaly | Asymmetrical skull |
| Turricephaly | Tower-shaped skull |
| Oxycephaly | Pointed skull |
4. Assessment of Head Size in Pediatrics
Head Circumference Measurement
Measured at largest occipitofrontal circumference.
Normal Head Circumference Growth
| Age | HC |
| -------- | -------- |
| Birth | 34–35 cm |
| 3 months | 40 cm |
| 6 months | 43 cm |
| 1 year | 46 cm |
| 2 years | 48 cm |
Growth Pattern
- First 3 months: ~2 cm/month
- 3–6 months: ~1 cm/month
- 6–12 months: ~0.5 cm/month
5. Red Flag Signs in Head Abnormalities
Urgent evaluation required if:
- Rapid head enlargement
- Bulging fontanelle
- Persistent vomiting
- Developmental regression
- Seizures
- Signs of raised intracranial pressure
If you want, I can also give 30–40 MCQs on abnormal head size and shape in pediatrics for exam preparation (NEET-PG / FMGE / NEXT level).