Larynx
Definition
The larynx is a hollow, fibrocartilaginous organ of the upper respiratory tract located in the anterior neck opposite C3–C6 vertebrae. It connects the laryngopharynx to the trachea and is essential for phonation, respiration, and protection of the lower airway.
Functions
- Phonation – production and modulation of voice
- Respiration – maintains a patent airway
- Airway protection – prevents aspiration during swallowing
- Cough reflex – expulsion of foreign bodies
Development
- Develops from the laryngotracheal diverticulum (endoderm)
- Cartilages and muscles arise from 4th and 6th pharyngeal arches
- Epiglottis develops from 3rd and 4th arches
External Features
- Laryngeal prominence (Adam’s apple) – prominent in males
- Thyroid notch
- Cricothyroid membrane – important for emergency airway access
Framework of Larynx
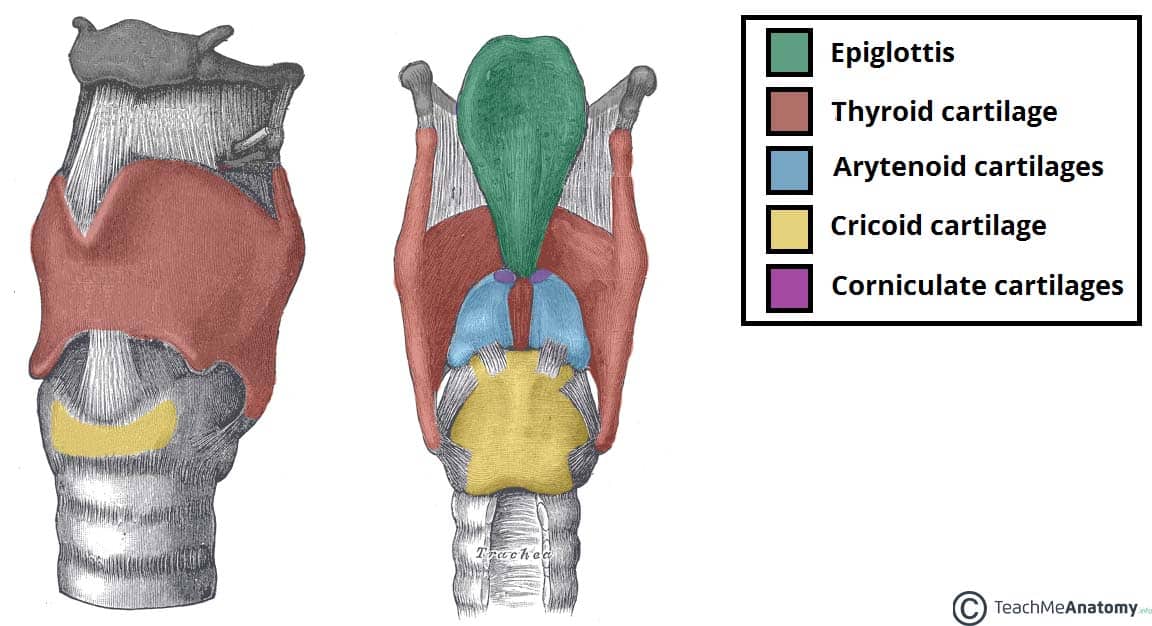
Laryngeal Cartilages
Unpaired (3)
- Thyroid cartilage
* Largest cartilage, two laminae forming laryngeal prominence
* Superior and inferior horns (cornua)
- Cricoid cartilage
* Complete ring (signet-ring shaped)
* Only complete cartilaginous ring in airway
* Lies at C6 level
- Epiglottis
* Leaf-shaped elastic cartilage
* Prevents food entering airway during swallowing
Paired (3)
- Arytenoid cartilages
* Pyramidal, sit on cricoid lamina
* Vocal process (vocal ligament attachment)
* Muscular process (muscle attachment)
- Corniculate cartilages
* Sit on arytenoids
* Support aryepiglottic folds
- Cuneiform cartilages
* Embedded in aryepiglottic folds
* Provide structural support
Joints of Larynx
- Cricothyroid joint
* Rotation and gliding
* Alters pitch by tensing vocal cords
- Cricoarytenoid joint
* Sliding and rotation
* Abduction and adduction of vocal cords
Ligaments and Membranes
- Thyrohyoid membrane – connects larynx to hyoid
- Cricothyroid membrane – access point for cricothyrotomy
- Quadrangular membrane – forms vestibular folds
- Conus elasticus – forms vocal ligaments
Cavity of Larynx
Divisions
- Vestibule
* From laryngeal inlet to vestibular folds
- Ventricle
* Space between vestibular and vocal folds
* Contains saccule (lubricates vocal cords)
- Infraglottic cavity
* From vocal folds to lower border of cricoid
Laryngeal Inlet (Aditus)
- Anterior – epiglottis
- Posterior – interarytenoid fold
- Lateral – aryepiglottic folds
Folds of Larynx
- Vestibular folds (false cords) – protective, no phonation
- Vocal folds (true cords) – phonation
* Stratified squamous epithelium
* White due to avascularity
Muscles of Larynx
Extrinsic Muscles
Move larynx up or down
Elevators
- Digastric
- Stylohyoid
- Mylohyoid
- Geniohyoid
Depressors
- Sternohyoid
- Sternothyroid
- Thyrohyoid
- Omohyoid
Intrinsic Muscles
Control vocal cord movement
| Muscle | Action |
| ------------------------------- | -------------------------------- |
| Posterior cricoarytenoid | Only abductor of vocal cords |
| Lateral cricoarytenoid | Adduction |
| Transverse & oblique arytenoids | Adduction |
| Cricothyroid | Tenses cords (raises pitch) |
| Thyroarytenoid | Relaxes cords (lowers pitch) |
| Vocalis | Fine tuning of voice |
Nerve Supply (Vagus Nerve)
Motor
- Recurrent laryngeal nerve (all intrinsic muscles except one)
- External laryngeal nerve → Cricothyroid
Sensory
- Internal laryngeal nerve – above vocal cords
- Recurrent laryngeal nerve – below vocal cords
Blood Supply
Arteries
- Superior laryngeal artery (from superior thyroid artery)
- Inferior laryngeal artery (from inferior thyroid artery)
Veins
- Superior and inferior laryngeal veins → thyroid venous plexus
Lymphatic Drainage
- Above vocal cords → Upper deep cervical nodes
- Below vocal cords → Lower deep cervical nodes
- Vocal cords themselves have poor lymphatic drainage
Surface Anatomy
- Upper border: opposite C3
- Lower border: opposite C6
- Moves upward during swallowing
Applied Anatomy
- Hoarseness – vocal cord pathology or recurrent laryngeal nerve injury
- Bilateral recurrent laryngeal nerve injury – airway obstruction
- Unilateral injury – hoarseness
- Cricothyrotomy – emergency airway access
- Laryngeal carcinoma – early hoarseness (glottic tumors)