Hypothyroidism – Complete Clinical Review
1. Definition
Hypothyroidism is a clinical syndrome caused by deficient thyroid hormone action at tissue level, resulting from inadequate production, secretion, transport, or peripheral action of thyroxine (T4) and triiodothyronine (T3).
2. Classification
A. Primary Hypothyroidism (≈95%)
Failure of the thyroid gland itself → ↑ TSH, ↓ Free T4
B. Secondary Hypothyroidism
Pituitary failure → ↓ or inappropriately normal TSH, ↓ Free T4
C. Tertiary Hypothyroidism
Hypothalamic TRH deficiency
D. Subclinical Hypothyroidism
↑ TSH with normal Free T4
E. Congenital Hypothyroidism
Absent or dysfunctional thyroid at birth
3. Etiology / Causes
Primary Causes
- Autoimmune
* Hashimoto thyroiditis (most common worldwide)
- Iatrogenic
* Thyroidectomy
* Radioiodine therapy
- Iodine imbalance
* Deficiency (endemic regions)
* Excess iodine (Wolff–Chaikoff effect)
- Drugs
* Amiodarone
* Lithium
* Interferon-α
* Tyrosine kinase inhibitors
- Thyroiditis
* Subacute (De Quervain)
* Postpartum thyroiditis
- Infiltrative
* Amyloidosis, sarcoidosis
- Radiation to neck
Secondary / Tertiary Causes
- Pituitary adenoma
- Pituitary surgery or irradiation
- Sheehan syndrome
- Craniopharyngioma
- Hypothalamic tumors
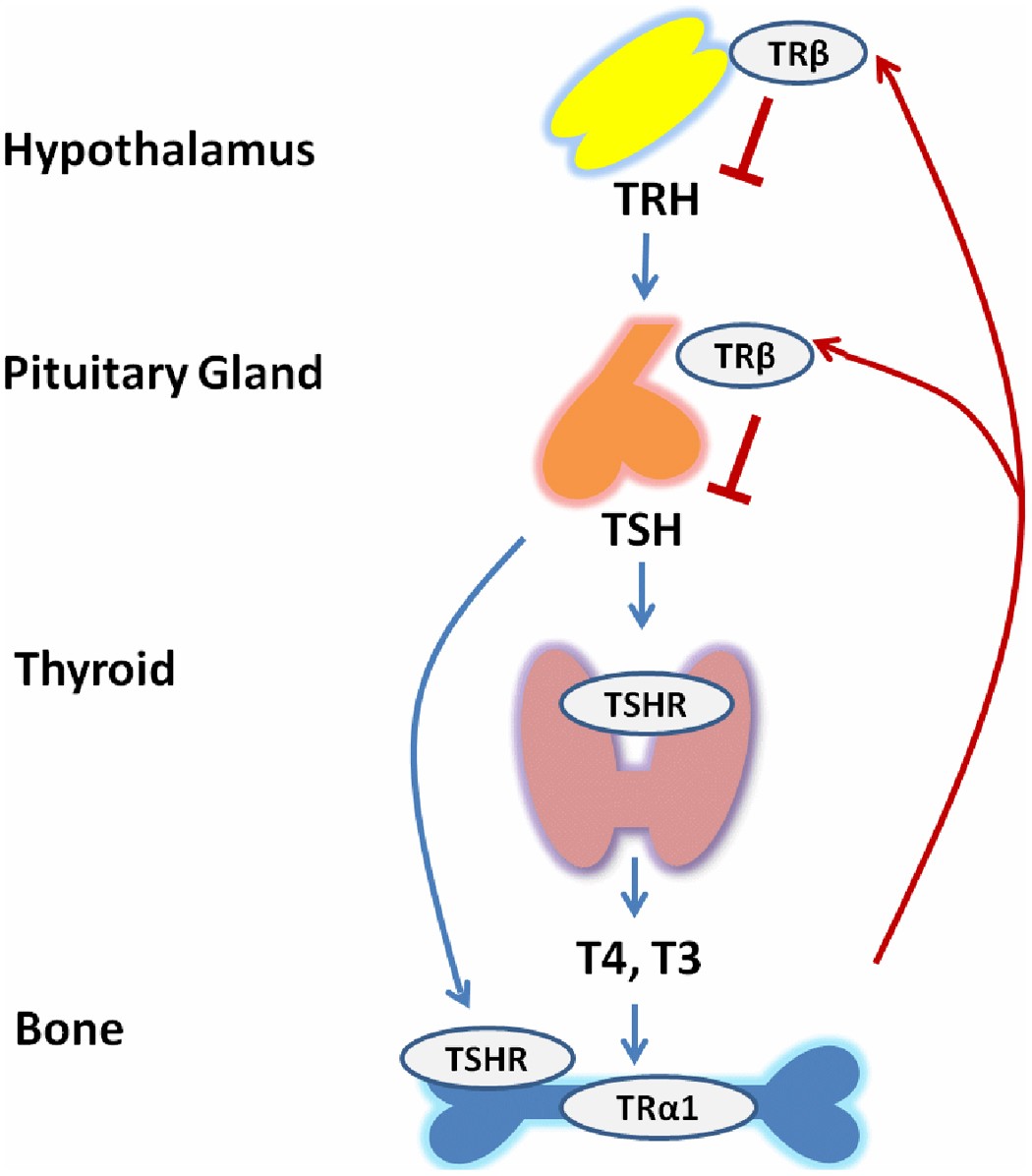
4. Pathophysiology
- Reduced thyroid hormone → ↓ basal metabolic rate
- ↓ mitochondrial oxidative metabolism
- Accumulation of glycosaminoglycans → myxedema
- ↓ adrenergic activity
- ↓ cardiac output and oxygen consumption
- Altered lipid metabolism → hypercholesterolemia
5. Clinical Features
A. General
- Fatigue, lethargy
- Cold intolerance
- Weight gain (fluid > fat)
- Decreased appetite
B. Skin & Hair
- Dry, coarse, cold skin
- Pallor with yellowish tint (carotenemia)
- Hair thinning, loss of lateral eyebrows
- Brittle nails
C. Face & ENT
- Puffy face
- Periorbital edema
- Hoarse voice
- Macroglossia
D. Cardiovascular
- Bradycardia
- Decreased cardiac output
- Diastolic hypertension
- Pericardial effusion
E. Gastrointestinal
- Constipation
- Abdominal distension
- Paralytic ileus (severe)
F. Neuromuscular
- Proximal muscle weakness
- Delayed relaxation of deep tendon reflexes
- Carpal tunnel syndrome
G. Neuropsychiatric
- Depression
- Cognitive slowing
- Psychosis (myxedema madness)
- Somnolence
H. Reproductive
- Menorrhagia → later amenorrhea
- Infertility
- Decreased libido
I. Hematologic
- Normocytic or macrocytic anemia
- Reduced erythropoiesis
6. Special Populations
Elderly
- Apathy, confusion
- Weight loss (not gain)
- Often misdiagnosed as dementia
Pregnancy
- Increased risk of:
* Miscarriage
* Pre-eclampsia
* Neurocognitive impairment in fetus
7. Investigations / Diagnosis
Primary Tests
- TSH – most sensitive
- Free T4
Patterns
| Condition | TSH | Free T4 |
| ---------------------- | -------- | ------- |
| Primary hypothyroidism | ↑ | ↓ |
| Subclinical | ↑ | Normal |
| Secondary | Normal/↓ | ↓ |
Etiology Work-up
- Anti-TPO antibodies (Hashimoto)
- Anti-thyroglobulin antibodies
Additional Findings
- ↑ Total cholesterol & LDL
- Hyponatremia
- Elevated CK
- Anemia
- Hypoglycemia (rare)
Imaging (if indicated)
- Thyroid ultrasound (autoimmune disease)
- MRI pituitary (secondary causes)
8. Differential Diagnosis
- Depression
- Chronic fatigue syndrome
- Anemia
- Adrenal insufficiency
- Nephrotic syndrome
- Congestive heart failure
- Fibromyalgia
9. Management
A. Pharmacologic Treatment
1. Levothyroxine (L-T4) – Drug of Choice
Indication
- All overt hypothyroidism
- Subclinical hypothyroidism if:
* TSH >10 mIU/L
* Symptomatic
* Pregnant
* Positive anti-TPO antibodies
Mechanism of Action
- Synthetic T4 → converted to T3 in peripheral tissues
- Restores normal metabolic activity
Usual Dosing
- Adults:
* 1.6 µg/kg/day (young, healthy)
- Elderly / CAD:
* Start 12.5–25 µg/day, titrate slowly
- Pregnancy:
* Increase dose by 25–30%
- Children:
* Higher weight-based dosing
Administration
- Empty stomach, morning
- Avoid food for 30–60 minutes
- Separate from calcium/iron by ≥4 hours
Pharmacokinetics
- Oral bioavailability: ~70–80%
- Half-life: ~7 days
- Hepatic metabolism
- Peripheral deiodination to T3
Adverse Effects (Overdose)
- Palpitations
- Tremor
- Weight loss
- Osteoporosis
- Atrial fibrillation
Contraindications
- Untreated adrenal insufficiency
- Acute MI (relative)
Drug Interactions
- ↓ Absorption: iron, calcium, PPIs, cholestyramine
- ↑ Clearance: phenytoin, carbamazepine, rifampicin
- Estrogens ↑ dose requirement
Monitoring
- TSH every 6–8 weeks after initiation or dose change
- Once stable → every 6–12 months
Patient Counselling
- Lifelong therapy in most cases
- Do not stop abruptly
- Consistent brand preferred
- Inform physician before pregnancy or new drugs
2. Liothyronine (T3)
- Not routinely recommended
- Used rarely in:
* Myxedema coma (IV)
* Selected refractory cases
B. Non-Pharmacologic Measures
- Adequate iodine intake (not excess)
- Balanced diet
- Weight management
- Cardiovascular risk reduction
- Treat anemia and dyslipidemia
10. Myxedema Coma (Medical Emergency)
Features
- Hypothermia
- Altered sensorium
- Bradycardia
- Hypoventilation
- Hyponatremia
Management
- ICU care
- IV levothyroxine ± liothyronine
- IV hydrocortisone (rule out adrenal crisis)
- Passive rewarming
- Ventilatory support
11. Prognosis
- Excellent with appropriate treatment
- Symptoms improve over weeks
- Lipids normalize in 2–3 months
- Lifelong follow-up required
12. Key Clinical Pearls
- Always rule out adrenal insufficiency before starting therapy
- Subclinical hypothyroidism is not always treated
- TSH is unreliable in secondary hypothyroidism—use Free T4
- Over-replacement is as harmful as under-treatment